 |
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Preface
Between 1993 and 1997, the World Health Organization (WHO) published the second edition of Guidelines for Drinking-Water Quality in three volumes: Volume 1: Recommendations (1993); Volume 2: Health Criteria and Other Supporting Information (1996); and Volume 3: Surveillance and Control of Community Supplies (1997). As with the first edition of the Guidelines, their development was organised and carried out jointly by WHO headquarters and the WHO Regional Office for Europe.
This pack is intended to provide information for use in the planning and delivery of seminars, workshops and training courses in water quality surveillance, control and improvement, especially where these concern the WHO Guidelines for Drinking-Water Quality. The pack contains 23 different sessions, including both presentation and practical exercises.
It is hoped that the availability of this pack will encourage and assist local, national and regional authorities to implement events of this type with or without the assistance of expert institutions or individuals. It is hoped that the pack will facilitate the development of expertise and thereby promote the organisation of further events.
The pack is designed to cover a broad range of water-related topics in order that appropriate elements can be selected in response to local circumstances and priorities. The pack includes sessions addressing the scientific basis of the Guidelines; the establishment of national standards; the ways in which water supplies may be improved; and some broader issues such as human resource development.
Each section of the pack addresses a single session and includes the objectives, a session plan, a background paper and overhead transparencies. The materials are intended to provide a resource person with information to assist in the review of what they might reasonably expect to achieve in a session, and to plan the structure and layout of the session. The background papers can, where appropriate, be provided to participants. The pack also addresses practical sessions. The materials provided to support these give guidance as to how such sessions could be delivered and the materials required to implement them.
It is unlikely that all sessions would be necessary for a single seminar, workshop or training course. It is therefore important that the overall objectives of an event are defined, taking local priorities into account when selecting which sessions will be of most practical use.
The sessions in the pack can be divided into a number of groups which could be of value when planning its use, defining the target audience and selecting sessions. The groups are described in the table over leaf.
In order to develop a well-balanced seminar, workshop or training course, at least one session would normally be required from each group. Discussion of drinking-water quality and the use of the Guidelines for Drinking-Water Quality should, for example, generally be accompanied by sessions considering monitoring and assessment and the means to secure improvements; and, possibly, a practical session illustrating issues of particular local relevance.
| |
Group |
Session Title |
|
1 |
Introduction |
Water and public health; |
|
2 |
The Guidelines |
Microbiological aspects; |
|
3 |
Monitoring and assessment |
Monitoring and assessment of microbiological
activity; |
|
4 |
Technical aspects |
Source protection; |
|
5 |
Organisational aspects |
Institutional frameworks; |
|
6 |
Practical exercises |
Microbiology; |
It is hoped that this pack will be a useful addition for those implementing training courses in water quality. The pack should assist in building capacities to provide and facilitate initial, further and ongoing training for staff of diverse disciplines. Any comments that users of the pack may have on experience with its use and which might assist in its further development would be gratefully received and should be addressed to:
Jamie Bartram
WHO
Water and Sanitation for Health Unit
1211 Geneva 27
Switzerland
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Water and Public Health
Session Objectives
· To demonstrate the link between water and health and show the profound influence of water supply and quality on public health.· To describe the basic classification of water-related disease.
· To describe the concept of the faecal-oral route of disease transmission and the classic waterborne disease cycle.
· To describe how improvements in water supplies will lead to improvements in health and a reduction in morbidity and mortality rates.
Introduction
Water has a profound influence on human health. At a very basic level, a minimum amount of water is required for consumption on a daily basis for survival and therefore access to some form of water is essential for life. However, water has much broader influences on health and wellbeing and issues such as the quantity and quality of the water supplied are important in determining the health of individuals and whole communities.
The first priority must be to provide access for the whole population to some form of improved water supply. However, access may be restricted by low coverage, poor continuity, insufficient quantity, poor quality and excessive cost relative to the ability and willingness to pay. Thus, in terms of drinking-water, all these issues must be addressed if public health is to improve. Water quality aspects, whilst important, are not the sole determinant of health impacts.
The quality of water does, however, have a great influence on public health; in particular the microbiological quality of water is important in preventing ill-health. Poor microbiological quality is likely to lead to outbreaks of infectious water-related diseases and may causes serious epidemics to occur.
Chemical water quality is generally of lower importance as the impact on health tend to be chronic long-term effects and time is available to take remedial action. Acute effects may be encountered where major pollution event has occurred or where levels of certain chemicals are high from natural sources, such as fluoride, or anthropogenic sources, such as nitrate.
Microbiological drinking-water quality and human health
The microbiological quality of drinking-water has been implicated in the spread of important infectious and parasitic diseases such as cholera, typhoid, dysentery, hepatitis, giardiasis, guinea worm and schistosomiasis.
Many other diseases are associated with water in other ways. Water may act positively in the control of some through its use in hygiene, and may act as a source or vector for others where contact with water is required for disease transmission or where agents of disease or insect vectors require water in which to complete their life cycle. The various relationships between water and disease are summarized in Table 1.
Water-related disease incidence worldwide
Water-related disease places an excessive burden on the population and health services of many countries worldwide and in particular those in developing countries. Table 2 shows estimates of the morbidity and mortality rates of some major water-related diseases worldwide, figures which are likely to be conservative estimates.
Table 1: Diseases related to water and sanitation
|
Group |
Disease |
Route leaving host |
Route of infection |
|
Diseases which are often water-borne |
Cholera |
faeces |
oral |
| |
Typhoid |
faeces/urine |
oral |
| |
Infectious hepatitis |
faeces |
oral |
| |
Giardiasis |
faeces |
oral |
| |
Amoebiasis |
faeces |
oral |
| |
Dracunculiasis |
cutaneous |
percutaneous |
|
Diseases which are often associated with poor hygiene |
Bacillary dysentery |
faeces |
oral |
| |
Enteroviral diarrhoea |
faeces |
oral |
| |
Paratyphoid fever |
faeces |
oral |
| |
Pinworm (Enterobius) |
faeces |
oral |
| |
Amoebaisis |
faeces |
oral |
| |
Scabies |
cutaneous |
cutaneous |
| |
Skin sepsis |
cutaneous |
cutaneous |
| |
Lice and typhus |
bite |
bite |
| |
Trachoma |
cutaneous |
cutaneous |
| |
Conjunctivitis |
cutaneous |
cutaneous |
|
Diseases which are often related to inadequate sanitation |
Ascariasis |
faecal |
oral |
| |
Trichuriasis |
faecal |
oral |
| |
Hookworm (Ancylostoma/Necator) |
faecal |
oral/percutaneous |
|
Diseases with part of life cycle of parasite in water |
Schistosomiasis |
urine/faeces |
percutaneous |
|
Diseases with vectors passing part of their life cycle in water |
Dracunculiasis |
cutaneous |
percutaneous |
adapted from Bradley, D J, London School of Hygiene and Tropical Medicine, various
Forty per cent of mortality in children under five years of age is related to diarrhoeal disease and it has been estimated that in 1995 more than 1,500,000,000 episodes of diarrhoea occurred in children under five years of age in the developing world (excluding China) and that some 4,000,000 of these resulted in death.
Table 2: Morbidity and mortality rates of some important water-related diseases (after WHO, 1995)
|
Disease |
Cases per year |
Deaths per year |
|
Cholera |
384 |
11 |
|
Typhoid |
500 |
25 |
|
Giardiasis |
500 |
low |
|
Amoebiasis |
48,000 |
110 |
|
Diarrhoeal disease |
1,500,000 |
4,000 |
|
Ascariasis |
1,000 |
20 |
|
Trichuriasis |
100 |
low |
|
Ancylostoma |
1,500 |
60 |
|
Dracunculiasis (Guinea worm) |
> 5,000 |
- |
|
Schistosomiasis |
200,000 |
800 |
|
Trachoma |
360,000 (active) |
9,000 (blind) |
These diseases are caused by the ingestion of contaminated faecal material transmitted by the transmitted by the faecal - oral route. Infectious agents of all types may be transmitted by the faecal - oral route via water, including viruses (such as infectious hepatitis, rotavirus and Norwalk agent); bacteria (such as cholera, typhoid and dysentery); and parasites (such as Giardia, Cryptosporidium and Entamoeba).
Faecal pollution of drinking-water may be sporadic and the degree of faecal contamination may be low or fluctuate widely. In communities where contamination levels are low, supplies may not carry life-threatening risks and the population may have used the same source for generations. However, where contamination levels are high, consumers (and especially the visitors, the very young, the old and those suffering from immuno deficiency-related disease, for instance through malnutrition or AIDS) may be at a significant risk of infection.
Improving water and sanitation and improvements in health
Results of epidemiological studies into the relationship between the quality of water supply and sanitation versus human health vary widely and there are severe methodological difficulties involved in undertaking such studies. Nevertheless there is sufficient evidence to support the conclusion that improving water supply and sanitation can have a significant impact on human health. Table 3 summarizes the findings of an extensive review of studies of this type.
Table 3: Percentage reduction in the diarrhoea morbidity rate attributed to improvements in water supply or excreta disposal
|
Type of Intervention |
Number of Studies |
Percentage reduction |
Range |
|
All |
53 |
22 |
0-100 |
|
Water quality improvements |
9 |
16 |
0-90 |
|
Improvements in availability |
17 |
25 |
1-100 |
|
Improvements in availability and quality of water |
8 |
37 |
0-82 |
|
Improvements in excreta disposal |
10 |
22 |
0-48 |
Source: after Esrey, Feachem and Hughes, 1985
One of the reasons for the difficulty in undertaking studies on the health impact of improvements in water supply quality is that the faecal - oral route includes several and multiple routes to infection as summarized in Figure 1 below.
Figure 1: Principal elements of
faecal - oral disease transmission
This complexity of routes also demonstrates the importance of various aspects of hygiene as complementary actions to water quality improvements.
Clearly, the likelihood of acquiring a waterborne infection increases with the level of contamination by pathogenic (disease-causing) microorganisms. However, the relationship is not necessarily a simple one and depends very much on factors such as infectious dose and host susceptibility.
Moreover there remains some doubt as to the relative importance of drinking-water quality and other aspects of water supply on the prevalence of infections with a faecal-oral route of transmission. For example, some agents with a low infectious dose may be transmitted primarily from person to person and thus improving the quality of drinking-water may not make a dramatic impact on their prevalence in the community. Human rotavirus and some species of Shigella fall into this category. Bacteria which are capable of multiplication in food may follow a food-borne transmission route more readily than waterborne.
Conversely there are other agents for example Salmonella typhi, Vibrio cholerae, Giardia lamblia and hepatitis A virus which are frequently transmitted via contaminated drinking-water. Where this is the case, improvements in water quality may result in substantial reductions in prevalence.
In those cases where transmission is not primarily water borne, improvements in water availability and personal hygiene may be much more important in reducing morbidity from diarrhoea and other water-borne infections.
The relative importance of drinking-water quality to the maintenance of public health may vary with respect to a number of geographical, social, seasonal and microbiological factors. It is not possible to state with any confidence which aspect of water supply is the most important at any one time or in any one location. What is becoming increasingly clear however is that all factors relating to the quality and availability of drinking-water are potentially important and must be taken into consideration. In this context it is worth emphasizing that one of the few general conclusions that may be drawn about drinking-water quality is that if faecally-derived pathogens are not present, then endemic or epidemic waterborne disease will not occur.
Other aspects of microbiological quality
As noted above, water borne disease is not exclusively transmitted by the faecal-oral route, although this route of disease transmission is of overwhelming importance globally. Some other microbiological aspects of importance are as follows:
Opportunistic and other water-associated pathogens
Opportunistic pathogens are naturally present in the environment and normally present no risk to human health. They are able to cause disease in people with impaired local or general immune defences. These people include the elderly and the very young; persons with extensive burns; persons undergoing immuno-suppressive therapy (such as following transplant surgery) and those with immuno deficiency-related diseases (such as AIDS). Examples of opportunistic pathogens of this type include Pseudomonas aeruginosa, certain species of Flavobacterium, Acinetobacter, Klebsiella, Serratia, Aeromonas and some 'slow growing' mycobacteria.
Inhalation of water containing certain infectious agents may also cause disease. This is the case with, for example, Legionella spp (Legionnaire's disease) and Naeglaria fowleri (an occasional cause of primary amoebic meningoencephalitis).
Cyanobacterial Toxins
Some cyanobacteria ('blue-green algae') are capable of producing toxins, including hepatotoxins, neurotoxins and lipopolysaccharides. Few epidemiological studies have been undertaken and little information is available regarding the true importance of this problem. Where blooms of cyanobacteria occur in lakes and reservoirs used for drinking-water supply a potential risk to health exists and therefore impounded surface waters used for drinking-water supply should be protected from contamination with nutrients.
Nuisance organisms
A number of organisms of no public health significance are undesirable because they produce turbidity, taste or odour or because they are visible to consumers of drinking-water. Their presence indicates that water treatment and supply system maintenance may be defective. These include: tastes and odours from Actinomyces and Cyanobacteria; and infestation of water mains by animal life feeding upon microbial films, such as the crustacean Gammarus pulex, Nais worms and the larvae of chironomids.
Chemical contamination and health
Chemical contamination of drinking-water may also have effects on health, although in general these tend to be chronic rather than acute, unless a specific pollution event has occurred and are therefore generally considered of lower priority than microbiological contamination.
Chemical pollutants which affect health include nitrate, arsenic, mercury and fluoride. In addition, there are an ever-increasing number of synthetic organic compounds released into the environment whose effect on human health is poorly understood, but which it appears may be carcinogenic.
Some details are given below on the four substances noted above, however, it must be recognized that raised concentrations of any chemical known to have an impact on human health may lead to long-term problems. In general, water sources used for drinking-water supply should be protected from chemical contamination through land-use control, definition of protection zones and application of adequate wastewater treatment.
Nitrate
Excess nitrate in drinking-water has been linked to methaemaglobinamenia in infants, the so-called 'blue-baby' syndrome. Nitrate leads to the oxidation of normal haemoglobin to methaemoglobin which is unable to transport oxygen to the tissues. This may result in cyanosis (a dark blue coloration) and in some cases, asphyxiation and death.
The Guideline Value (GV) for nitrate of 50 mg/l has been set on the basis of the acute health risk to infants and is unusual for this reason as most GVs are set for long-term risks. Many countries are now experiencing problems with elevated nitrate, particularly in groundwaters caused through poor treatment and disposal of excreta, intensification of animal husbandry and large-scale applications of inorganic and organic fertilizers.
In some countries, notably in the Countries of Central and Eastern Europe (CCEE) such as Moldova and Romania, levels have been recorded in shallow groundwater at up to 1000 mg/l, whilst in India anecdotal evidence suggest levels of up to 1500 mg/l. At these levels, more widespread chronic effects are likely to be noted including a possible greater likelihood of gastric cancer.
Nitrate is a conservative element in natural groundwaters and therefore once large-scale nitrate contamination has occurred, it will take a considerable period of time before it is naturally attenuated through de-nitrification or diluted. In these circumstances, short term measures will include identifying alternative sources of water, for instance deeper boreholes, or through blending with low-nitrate waters. Removal of nitrate by ion exchange in treatment plants is expensive as most anion exchangers are non-selective for nitrate and therefore nitrate specific resins must be used.
Long-term solutions must involve the reduction in the release of nitrate into the environment through, for example, control of fertilizer application and improvements in human and animal excreta treatment and disposal.
Arsenic
A provisional GV of 0.1 mg/l has been set for arsenic on the basis of an excess cancer risk of 6 × 10-4. In some parts of the world, natural sources of arsenic may contaminate water supplies and lead to poisoning of the users. The most well-documented cases of arsenic poisoning from drinking-water have come from India, where there is arsenic contamination of large numbers of rural water supplies. Common symptoms include inflamed eyes and skin lesions. Arsenic contamination has also been noted in southern Thailand and the CCEE.
Most natural arsenic comes from the reduction of arsenic complexes caused through changing redox and pH conditions and from the oxidation of arsenic containing minerals exposed by falling groundwater tables induced through over abstraction or reduced recharge.
There is also increasing evidence that there is a tendency for arsenic levels to increase in shallow groundwaters under urban areas. This has been particularly noted where conditions become anoxic, organic rich sediments are present and arsenate compounds associated with iron are common. This has significant implications for water supply in these areas, particularly in low-income areas where community-based water projects may involve the sinking of dug and wells and shallow tube wells. Arsenic may also be discharged in effluent from a variety of industrial processes.
Control options for arsenic contamination will vary according to the source. Arsenic derived from industrial effluents should be controlled through proper treatment of wastes and monitored by the pollution control agency. The control of arsenic from natural sources must include sustainable groundwater resource management. Many of the problems noted in India result from over-abstraction of groundwater, primarily by the agricultural sector. Arsenic problems noted under urban areas may be more difficult to control given the range of factors which influence whether arsenic is released.
In all cases, short-term options will include treatment of water in home using, use of alternative sources or a switch to an alternative source, such as deep groundwater unaffected by arsenic contamination. Arsenic may be removed at treatment plants through a variety of processes, although like most treatment aimed at chemical removal, increase the costs of producing drinking-water.
Fluoride
Fluoride in drinking-water can have toxic effects in both excess and deficiency, although WHO only set a GV of 1.5 mg/l for excess fluoride as susceptibility in deficiency is highly dependent on nutritional status.
Excess fluoride may lead to dental or skeletal fluorosis, the latter being a crippling disease which affects a number of areas including the Rift valley of East Africa and parts of India, Mexico and the former Soviet Union. However, a lack of fluoride may cause dental caries, a weakening of the teeth, thus in some circumstances fluoride may be added to the drinking-water supply.
The acceptable concentration of fluoride in water is in part related to climate, as in warmer climates the quantities of water consumed are higher thus leading to a greater risk of fluoride related problems as overall intake increases. Susceptibility of individuals to fluorosis may also be determined by renal impairment.
Control options for fluoride contamination of water include blending of fluoride-rich waters with waters of low fluoride content, selection of low-fluoride sources and removal of fluoride by treatment at public water supply or household level. Fluoride can be successfully removed by precipitation by use of coagulants (commonly an alum-lime mix), adsorption on activated carbon substrates, osmosis or ion exchange. Fluoride removal is often more effective at a water supply level and the Nalgonda technique, developed in India, has been proven as a low-cost techniques which can operate on a variety of water supply options ranging from piped water supplies to handpump units.
References
Anon. World Health Organization Guidelines for Drinking-water Quality, Volume I, 2nd Edition, WHO, Geneva, 1993
Anon., World Health Organization Guidelines for Drinking-water Quality, Volume II, 2nd Edition, WHO, Geneva, 1996 Anon. Report of a National Water Quality Seminar, Romania, WHO-EURO, Rome, 1995
Esrey, S.A., Feacham, R.G. & Hughes, J.M., Interventions for the control of diarrhoeal diseases among young children: improving water supplies and excreta disposal facilities, Bulletin of the World Health Organization, vol. 63, No. 4, pp. 757-772, 1985.
Hofkes, E.H. (Ed), Small Community Water Supplies, John Wiley & Sons. Chicester. 1986.
Presentation Plan
|
Section |
Key points |
OHP |
|
Introduction |
· water has a profound influence on health, at the most basic level this means that a minimum amount is required for consumption each day for survival |
1 |
| |
· the influence of water on health goes far beyond this as water is a principal medium for disease prevention | |
| |
· WHO recognises that access to adequate water supplies is a fundamental human right | |
| |
· this was confirmed at the Mar del Plata conference in 1977 |
|
|
Water-related disease incidence |
· water-related diseases account for over 80 per cent of all deaths in developing countries |
2 |
| |
· infectious and parasitic diseases are the major cause of morbidity in developing countries and cause important outbreaks world-wide |
|
|
|
· many of the water-related diseases lead to epidemics which may have relatively high mortality/morbidity ratio | |
|
Water supply improvements |
· improved water supply and sanitation will lead to reduced |
3,4 |
| |
· incidence of morbidity and mortality | |
| |
· this may be up to 100 per cent for some diseases such as typhoid or dracunculiasis | |
| |
· need improvements in water supply and sanitation to achieve these objectives as improvement in one aspect aloe will not produce the full health benefits expected | |
| |
· water quality is only one aspect of water supply that should be improved | |
| |
· increased coverage, continuity of supply and quantity of water supplied at a reasonable cost are all important | |
| |
· infant mortality rates (a key sentinel community) can be significantly reduced with improved water supply | |
|
Water-related disease types |
· very many water-related diseases |
5 |
| |
· not all water related diseases are fatal or lead to epidemics, but all debilitating to some degree | |
| |
· water-related diseases may be classified on the basis of transmission | |
| |
· the principal classes are: water-borne; water-washed; water based; and water-related insect vectors |
|
| |
· many infectious diseases can be classified in more than one group, for instance most diarrhoeal disease may be transmitted by a classic water-borne route, but are also related to inadequate quantities of water (hygiene) | |
|
Disease transmission |
· many diseases may be transmitted via the faecal-oral route |
6,7 |
| |
· these include infectious diseases such as cholera and hep A |
|
|
|
· transmission occurs when human faecal matter is ingested through drinking contaminated water or eating contaminated food | |
| |
· water is an important medium for transmitting disease as contamination with excreta can lead to ingestion of faecal matter(see infection cycle) |
|
Water Quality
"All people, whatever their stage of development and social and economic condition, have the right to have access to drinking water in quantities and of a quality equal to their basic needs."
(UN Conference at Mar del Plata, 1977)
Global Morbidity and Mortality Rates
| |
Number/Year or Total Reported | |
| |
Cases of disease |
Deaths |
|
Cholera |
384 000 |
11 000 |
|
Typhoid |
500 000 |
25 000 |
|
Giardiasis |
500 000 |
low |
|
Amoebiasis |
48 000 000 |
110 000 |
|
Diarrhoeal disease |
1 500 000 000 |
4 000 000 |
|
Dracunuliasis (guinea-worm) |
> 5 000 |
- |
|
Schistosomiasis |
200 000 000 |
800 000 |
World Health Report, 1995
Potential Reductions in Morbidity for Different Diseases as a Result of Improvements in Water Supply and Sanitation
|
Diseases |
Projected reduction in morbidity (%) |
|
Cholera, thyphoid |
80-100 |
|
Diarrhoeal diseases, dysentery, gastroenteritis |
40-50 |
|
Dracunuliasis |
100 |
|
Schistosomiasis |
60-70 |
Infant Mortality versus Access to
Safe Water
Source: Regli et. al 1993
Water and Sanitation-related Diseases
|
Group |
Diseases |
|
Water-borne diseases |
Cholera; Typhoid; Bacillary dysentery; Infectious hepatitis; Giardiasis |
|
Water-washed diseases |
Scabies; Skin sepsis and ulcers; Yaws; Leprosy; Lice and thypus; Trachoma; Dysenteries; Ascariasis; Parathphoid |
|
Water based diseases |
Schistomiasis; Dracunuliasis; Bilharziosis; Filariasis; Threadworm |
|
Water-related insect vector diseases |
Yellow fever; Dengue fever; Bancroftian filariasis; Malaria; Onchocerciasis |
The Faecal-Oral Route of Disease
Transmission
The Classical Waterborne Infection
Cycle
Source: Tebbutt, T.H.Y., 1992
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The WHO Guidelines for Drinking-Water Quality
Session Objectives
· To introduce the latest edition of the Guidelines; identifying all three volumes and the information contained within each.· To emphasise the basic concept and the advisory nature of the Guidelines and to describe the difference between scientific risk assessment and risk management.
· To provide an outline of the consultation process that resulted in the revised 2nd edition of the Guidelines.
· To discuss the reasoning behind the prioritisation of microbiological quality of drinking water in the Guidelines.
· To provide a basic overview of the criteria used in the selection of contaminant substances that are contained within the Guidelines.
· To explain the nature of Guideline Values, highlighting substances and parameters to which they apply.
· To explain the process of the rolling revision of the Guidelines.
Introduction
An established goal of WHO and its Member States is that:
all people, whatever their stage of development and their social and economic conditions have the right to have access to an adequate supply of safe drinking-water.
In this context, 'safe' refers to a water supply which is of a quality which does not represent a significant health risk, is of sufficient quantity to meet all domestic needs, is available continuously, is available to all the population and is affordable. These conditions can be summarised as five key words: quality; quantity; continuity; coverage; and, cost.
The importance of these key words cannot be over-emphasized since the impact of contaminated drinking-water on health has been well documented and range from massive outbreaks of infectious and parasitic diseases to subtle chronic toxicological effects. It is vital that all these key issues are addressed, if clear policies and programmes on water supply and quality are to be established and maintained.
To assist governments in dealing with these and related issues regarding water quality, WHO has over the years, been involved in the review and evaluation of information on health aspects of drinking-water supply and quality and in issuing guidance material on the subject.
The first WHO publication dealing specifically with drinking-water quality was published in 1958 as International Standards for Drinking-Water. It was subsequently revised in 1963 and in 1971 under the same title. Because of the ever-continuing research on water quality, the 1971 standards were again reviewed, and in 1984 the WHO Guidelines for Drinking-Water Quality were published.
The philosophy and content of these Guidelines constituted a significant departure from the old International Standards as they were designed as advisory in nature based solely on the impacts on human health of the various substances and organisms considered. Standards have, by their nature, to take other considerations into account such as social, economic, environmental, political and financial considerations and have to balance a number of criteria.
In 1989, work was started on a second edition of the Guidelines. These new Guidelines which were published in 1993-97 rely to a great extent on the pioneering concepts of the 1984 Guidelines.
The purpose of this paper is to briefly describe the second edition of the Guidelines, the revision process and the scope and new concepts incorporated into the Guidelines for the 1990s.
Presentation
The Guidelines have been published in three volumes:
Volume 1 - Recommendations describes the criteria used in selecting the various microbiological, chemical and radiological contaminants considered, the approaches used to derive the guideline values, and brief information supporting the values recommended, or explaining why no health-based guideline value was recommended.Volume 2 - Health Criteria and Other Supporting Information is essentially an environmental health criteria document covering the contaminants that were examined with a view to recommending guideline values. Volume 2 elaborates greatly on the health risk assessment of microbial and chemical contaminants presented in Volume 1 and should be considered as a vital companion document.
Volume 3 - Surveillance and Control of Community Supplies deals specifically with small communities, predominantly those in rural areas of developing countries.
Preparation
At the time the Guidelines for Drinking-Water Quality were published in 1984, it was recognized that as new information on the potential health risks of contaminants in drinking-water became available, the basis of the recommended guideline values would need to be reviewed and revised. New or changed guideline values would therefore have to be recommended.
In 1988, the decision was made within WHO to initiate the revision of the Guidelines. As with the 1984 Guidelines, responsibility for carrying out this revision was shared between WHO's Headquarters and the Regional Office for Europe (EURO). Within Headquarters, both the Urban Environmental Health Unit (UEH) and the International Programme on Chemical Safety (IPCS) were involved; IPCS providing a major input to the health risk assessment of chemicals in drinking-water.
From the onset, it was agreed that the general philosophy of the 1984 Guidelines remained sound and valid and should therefore not be changed.
A series of planning and co-ordination meetings took place to establish the scientific approach and mechanism for the preparation of evaluation documents, substance by substance, for the revision of the Guidelines. This was followed by a series of Review Group Meetings dealing with specific subject areas. A total of 19 meetings were held involving the participation of numerous institutions, and over 200 experts from some 40 different countries.
The preparation of the Guidelines required intensive human and financial resources. The Guidelines could not have been developed without the scientific and/or financial support of the following organisations and countries: DANIDA, NORAD, SIDA, ODA (UK), Belgium, Canada, Denmark, Finland, France, Germany, Italy, Japan, Netherlands, Norway, Poland, Sweden, United Kingdom, and the United States of America.
Microbial contaminants and some 128 chemicals were selected for evaluation. For each selected chemical, a lead country prepared a draft evaluation document examining its occurrence in drinking-water, exposure from food and air, effects on laboratory animals and humans. Based on the evaluation of available data, a guideline value was also proposed. The outline of such an evaluation document is given as Annex 1. These evaluations constitute Volume 2 of the Guidelines.
The draft evaluation document was then circulated for review by the Co-ordinator to the "support countries" and selected experts. The Co-ordinator worked with the lead countries to incorporate the comments received and prepared overviews of scientific issues to be resolved. This documentation was then submitted for evaluation to a Review Group meeting which took a decision as to the health risk assessment and recommended a guideline value. The role of the seven Co-ordinators was crucial in the revision process.
During the preparation of draft evaluation documents and at the Review Group meetings, careful consideration was always given to previous risk assessments carried out by the WHO/ILO/UNEP International Programme on Chemical Safety in its Environmental Health Criteria Monographs, by the International Agency for Research on Cancer, the Joint FAO/WHO Meeting on Pesticide Residues and the Joint FAO/WHO Expert Committee on Food Additives which also evaluates contaminants such as lead and cadmium in addition to food additives.
Basic Concept
As reflected in the title, the Guidelines are of an advisory nature and are intended to be used by national or regional authorities as a basis for the development of drinking-water standards and regulations appropriate to their own socio-economic and exposure situation. The Guidelines clearly recognize the desirability of adopting a risk-benefit approach (qualitative or quantitative) to national standards and regulations. The establishment of drinking-water quality standards by individual governments must follow a very careful process in which the health risk is considered alongside other factors, such as technical and economic feasibility. Standards achieve nothing unless they can be implemented and enforced. When establishing national standards, consideration must be given to the practical measures that will need to be taken with respect to finding new sources of water supply, instituting certain types of treatment, and providing for adequate surveillance and enforcement.
Priorities
Since water is essential to life, the first priority is that it must be made available to consumers even if the quality is not entirely satisfactory.
As with the 1984 Guidelines, the new 1993 Guidelines place the greatest emphasis on the microbiological quality of drinking-water. The microbial contamination of drinking-water has been implicated, directly or indirectly, in the spread of major infectious and parasitic diseases such as cholera, typhoid, dysentery, hepatitis, giardiasis and guinea-worm infection. In 1992, the United Nations Conference on Environment and Development (UNCED) estimated that '..80 per cent of all diseases, and over one-third of deaths in developing countries are water-associated, and on average as much as one-tenth of each person's productive time is sacrificed to water-related diseases' (Agenda 21, UNCED, Chapt. 18, p175). Diseases associated with water are heavily concentrated in the developing world, and within the developing world, among the poorer urban and rural households of the poorer countries.
Diseases arising from the ingestion of pathogens in contaminated water have the greatest impact worldwide. Table 1 shows the morbidity and mortality rates of the major water-related diseases. These figures provided to WHO by Member States are in many cases underestimated. For instance, no figures are available for certain diseases such as hepatitis which are often waterborne, some countries with numerous cases of typhoid do not report any to WHO, whilst others do not have the infrastructure to conduct the necessary surveys. There can be little doubt that true annual morbidity and mortality rates are well over these figures. It would be erroneous to ascribe these diseases exclusively to unsafe drinking-water. With the exception of dracunculiasis which is transmitted solely by drinking-water, a variety of non-water sources are also important.
Table 1: Morbidity and mortality rates of some important water-related diseases (after WHO, 1995)
|
Disease |
Cases per year |
Deaths per year |
|
Cholera |
384 |
11 |
|
Typhoid |
500 |
25 |
|
Giardiasis |
500 |
low |
|
Amoebiasis |
48,000 |
110 |
|
Diarrhoeal disease |
1,500,000 |
4,000 |
|
Ascariasis |
1,000 |
20 |
|
Trichuriasis |
100 |
low |
|
Ancylostoma |
1,500 |
60 |
|
Dracunculiasis (Guinea worm) |
> 5,000 |
- |
|
Schistosomiasis |
200,000 |
800 |
|
Trachoma |
360,000 (active) |
9,000 (blind) |
The toll of human suffering from the microbial contamination of drinking-water is indeed heavy. As with the 1984 Guidelines, the 1993 Guidelines, justifiably, stress protection of water supplies from microbial contamination and call for uncompromised disinfection of drinking-water despite the potential formation during this process of compounds with potentially harmful long-term health effects.
Selection Criteria
Thousands of organisms and substances have been identified in drinking-water supplies around the world. It is neither necessary nor feasible to develop recommendations for all these.
Microorganisms selected for evaluation were selected through an international consultation process, on the basis of the presence in water and likely risk to human health. Particular emphasis was given to developing guidance on selection of indicator organisms that can give early warning of faecal contamination and likely potential risks of disease. The Guidelines adopted a clear policy from the outset that microbiological quality must be the key water quality priority.
Chemicals for evaluation were selected through an international consultative process, guided by three main criteria:
· The substance presents a potential hazard for human health;· The substance was detected relatively frequently and at relatively high concentrations in drinking-water indicating that there may be significant exposure to humans;
· The substance was of major international concern (i.e. of interest to several countries).
On this basis, some 128 priority chemicals were selected for evaluation in the Guidelines and health-based acceptable levels of exposure from drinking-water (Guideline Values) recommended for 95 of these, taking into account all sources of exposure. Guideline values were not recommended for certain substances because they were found to be not hazardous to health, because of inadequate health effects information, or because the concentration of the chemical normally found in drinking-water does not represent a hazard to human health. Contaminants evaluated included chlorinated alkanes, ethylenes and benzenes, aromatic hydrocarbons, pesticides, inorganic chemicals, disinfectants and disinfectant by-products.
The Guideline Value
The recommendations made concerning water quality are expressed as Guideline values (GVs). Guideline values are not formal standards or regulatory limits and are not to be taken as strict limits such as "maximum permissible concentrations". They are intended to provide quantitative risk assessment information for regulatory authorities, risk managers, and others to make decisions concerning human health protection and to be adapted to national requirements and situations in prescribing limits and standards.
Guideline Values require adaptation because they relate to a "reference" human in a specified exposure environment. National populations and exposure situations will be different.
What is a guideline value?
· Guidelines are set for indicator bacteria - E.coli or thermotolerant (faecal) coliforms and total coliforms. These have been selected as they give a good indication of the likelihood of faecal contamination and the integrity of a water supply.· Unlike chemical guideline values, the presence of indicator bacteria will always represent a health risk. However, when faecal contamination is indicated, water supplies should not be closed off unless a better source of water is available for use. The microbiological Guidelines should be used as a desirable end-point and improvement in microbiological water quality should be the priority for water supply.
· A guideline value represents the concentration of a chemical constituent that does not result in any significant risk to the health of the consumer over a lifetime of consumption.
· Short-term deviations above the guideline values do not necessarily mean that the water is unsuitable for consumption. The amount by which, and the period for which, any guideline value can be exceeded without affecting public health depends upon the specific substance involved.
· Although the guideline values describe a quality of water that is acceptable for life-long consumption, the establishment of these GVs should not be regarded as implying the quality of drinking water may be degraded to the recommended level. Indeed, a continuous effort should be made to maintain drinking-water quality at the highest possible level.
· When a guideline value is exceeded, the authority responsible for public health should be consulted for advice on suitable action, taking into account the intake of the substance from sources other than drinking-water (for chemical constituents), and the practicability of remedial measures.
· When developing national drinking-water standards based on these guideline values, it will be necessary to take account of a variety of geographical, socioeconomic, dietary and other conditions affecting potential exposure. This may lead to national standards that differ appreciably from the guideline values.
The recommended GVs must be both practical and feasible to implement as well as protective of public health. Guideline values are therefore not set at concentrations lower than the detection limits achievable under routine laboratory operating conditions. Moreover, guideline values are recommended only when control techniques are available to remove or reduce the concentration of the contaminant to the desired level.
Contrary to the 1984 Guidelines, the 1993 Guidelines do not propose guideline values for substances and parameters that affect the acceptability of drinking-water to consumers. The Review Groups were of the opinion that guideline values should be recommended only for those substances that are directly relevant to health.
Many of the inorganic and aesthetic constituents evaluated in the Guidelines are known to be essential for life. No attempt was made in the Guidelines to define minimum desirable concentrations of essential elements in drinking-water.
Contaminants derived from water treatment chemicals, construction materials, paints or coatings were not specifically addressed. The control of such contaminants is best accomplished by appropriate specifications for and control of the quality of the products themselves rather than the quality of the water.
The recommended guideline values are set at a level to protect human health; they may not be suitable for the protection of aquatic life.
The Guidelines apply to bottled water and ice intended for human consumption but do not apply to natural mineral waters, which should be regarded as beverages rather than drinking-water in the usual sense of the word. The Codex Alimentarius Commission has developed Codex standards for such mineral waters.
Future Revision
Understanding of water quality and the health risk from microbes and chemicals is constantly increasing and the knowledge base expanding. As a result, it has been agreed that there will be a continuing process of updating of the Guidelines with a number of substances or agents subject for evaluation each year. New editions of the Guidelines will be published at about ten-year intervals. For the 3rd edition of the Guidelines, the protection and control of water quality will be prioritised and issues such as development of monitoring and assessment methodologies in urban areas, resource and source protection and control of chemicals and materials used in water treatment fully addressed. This will lead to the preparation of a volume 4 of the Guidelines, either as a single volume or in the form of a series of documents in the Guidelines series.
Biennial addenda to the Guidelines are to be issued, beginning in 1997 containing evaluations of new substances or substances already evaluated for which new scientific information has become available. Substances for which provisional guideline values have been established will receive high priority for re-evaluation. Table 2 overleaf summarises the priorities for the first addendum in 1997.
Table 2: Priorities for the first addendum, 1997
|
MICROBES |
CHEMICALS | |||
| |
Inorganics |
Organics |
Pesticides |
Disinfectants & DBPs |
|
Hepatitis A & E |
aluminium |
cyanobacterial toxins |
1,2-dichloropropane diquat |
chloroform |
|
Aeromonas spp. |
boron |
EDTA |
ethylene |
sodium |
|
Cyanobacteria |
copper |
PAHs |
pentachlorophenol |
|
|
Legionella spp. |
nickel | |
carbofuran | |
|
Vibrio cholerae |
nitrate & nitrite | |
2,4-D | |
|
Cryptosporidium parvum |
uranium | |
glycophosphate | |
|
Giardia lambia | | | | |
Conclusions
The Guidelines are based on international consensus assessment of the risks to human health from the presence of microbial and chemical contaminants in drinking-water and provide a sound scientific basis for establishing standards with respect to health protection.
It is the hope of the Organization that the Guidelines will be utilized by governments at all levels to set new drinking-water quality standards where they do not yet exist, or to update and expand existing ones. Thus, legislators and policy makers now have access to more comprehensive and detailed information to match health criteria with economic and technological when establishing drinking-water quality standards.
Table 1: Priorities for the first addendum, 1997
|
MICROBES |
CHEMICALS | |||
| |
Inorganics |
Organics |
Pesticides |
Disinfectants & DBPs |
|
Hepatitis A & E |
aluminium |
cyanobacterial toxins |
1,2-dichloropropane diquat |
chloroform |
|
Aeromonas spp. |
boron |
EDTA |
ethylene |
sodium |
|
Cyanobacteria |
copper |
PAHs |
pentachlorophenol |
|
|
Legionella spp. |
nickel | |
carbofuran | |
|
Vibrio cholerae |
nitrate & nitrite | |
2,4-D | |
|
Cryptosporidium parvum |
uranium | |
glycophosphate | |
|
Giardia lambia | | | | |
Presentation Plan
|
Section |
Key points |
OHP |
|
Introduction |
· an established goal of WHO is to ensure all population have access to an adequate water supply | |
| |
· WHO provides advice on health-related aspects of drinking-water | |
|
Guidelines presentation |
· Guidelines published in 3 volumes: |
1 |
| |
Volume I - recommendations | |
| |
Volume II - health criteria and other supporting information | |
| |
Volume III - small community water supplies | |
|
Guidelines presentation |
· when 1st edition of the Guidelines published in 1984, it was recognised that they would need updating |
2,3 |
| |
· 2nd edition published in 1993-97 | |
| |
· preparation went through a series of planning and co-ordination meetings to establish the scientific approach & mechanism; by review meetings | |
| |
· microbial contaminants and 128 chemicals selected for evaluation |
|
|
|
· for each microbe and chemical a lead country prepared draft document and, where appropriate, suggesting a preliminary guideline value (GV) |
|
|
|
· documents circulated to review group (over 200 scientists from 40 countries) and GVs revised and approved |
|
|
Basic concept |
· Guidelines are advisory In nature |
4 |
| |
· intended that GVs are used as a basis for establishing national and regional standards based on risk assessment and prevailing socio-economic conditions | |
| |
· the Guidelines stress the use of risk-benefit approaches to standard setting | |
| |
· standards must be developed which are achievable and enforceable; this may mean setting interim standards | |
|
Priorities for standards |
· access is key priority even where quality is inadequate |
5 |
| |
· the priority water quality concern is microbiological quality because of the link to health and acute disease | |
| |
· 1992, UNCED estimated >80% of all disease and >1/3 deaths in developing countries are caused by the consumption of contaminated water |
|
|
|
· disease associated with water heavily concentrated in less-industrialised countries in the poorer households in these countries | |
| |
· greatest impact on health is from ingestion of pathogens |
|
|
|
· available global figures on disease are likely to be underestimated | |
| |
· improvement in microbiological quality of water should lead to a reduction in disease incidence and severity | |
|
Selection criteria |
· major pathogens reviewed but no GVs set as routine surveillance of pathogens is not practical |
6,7 |
| |
· GVs set for indicator bacteria and operational parameters such as turbidity and chlorine residual | |
| |
· of 128 substances reviewed, GVs set for 95 | |
| |
· are not strict standards, but advisory guidelines | |
|
Guideline Values |
· provide quantitative risk assessment for authorities, but require adaptation as refer to reference human in specified exposure environment |
8,9 |
| |
· exceeding microbial GV indicates faecal contamination and therefore health risk | |
| |
· most chemical GV set for health risk from lifetime consumption | |
| |
· exceedance of chemical GV for short periods does not necessarily mean water unfit for consumption | |
| |
· no GV for aesthetic parameters | |
| |
· no minimum concentrations specified | |
| |
· do not address environmental/ecological concerns |
|
|
|
· do not specifically address treatment chemicals, construction materials etc. | |
| |
· do not apply to natural mineral waters | |
| |
· rolling revision started, with addenda published every 2 years |
|
|
Future developments |
starting 1997 |
10,11, Tab 1 |
| |
· 3rd edition will see greater emphasis on risk management |
|
|
|
· new Volume IV to be prepared on protection and control of water quality | |
| |
· GV based on international consensus of health risk | |
|
Conclusions |
· GV should be used to set or revise national/regional standards using a risk-benefit approach | |
| |
· Guidelines require continuous updating as knowledge increases |
|
WHO Guidelines for Drinking-water Quality
· Volume 1 - Recommendations
· Volume 2 - Health Criteria and other supporting information
· Volume 3 - Surveillance and control of community supplies

Consultation Process for Setting
Guideline Values (Part 1)
Consultation Process for Setting Guideline Values (Part 2)
|
Co-ordinators |
Review Meetings |
|
Microbiology |
2 |
|
Inorganics |
2 |
|
Organics and pesticides |
4 |
|
Disinfectants and by-products |
1 |
|
Radionuclides |
1 |
|
Volume 3 |
2 |
|
Planning consultations |
4 |
|
Other consultations |
3 |
|
TOTAL |
19 |
What is a Guideline Value?
· For microbes: no significant risk of pathogen presence at infectious dose.· For most chemicals: no significant risk to health over a lifetime of consumption.
· Some chemicals (e.g. nitrate): no significant risk of acute intoxication of vulnerable group.
· National standards may be appreciably different from guideline values.
Priority Microbes considered in the GDWQ
· Orally transmitted pathogens of high priority (microbes associated with human faeces)· Opportunistic and other water associated pathogens (moderate priority)
· Toxins from cyanobacteria
· Nuisance organisms causing rejection
· Guideline values for indicator bacteria and operational parameters
Selection Criteria
1. Adverse effects
2. Magnitude, frequency and duration of exposure
3. Population exposed
4. International concern
IARC Groups
|
Group 1: |
The agent is carcinogenic to humans |
|
Group 2A: |
The agent is probably carcinogenic to humans |
|
Group 2B: |
The agent is possibly carcinogenic to humans |
|
Group 3: |
The agent is not classifiable as to its carcinogenicityto humans |
|
Group 4: |
The agent is probably not carcinogenic to humans |
IARC overall evaluation of chlorinated drinking-water: Group 3
Guideline Values
· No GV for individual pathogens: use indicator bacteria, turbidity and chlorine residual· No GV for aesthetic parameters
· Treatment chemicals and construction materials not addressed
· No environmental effects
· Not for mineral water
· No minimum desirable level
Provisional Guideline Values
· Limited health effects information and/or UF>1000· Health-based GV below quantitation level
· Health-based GV cannot be achieved through practical treatment methods
· Disinfection likely to result in health-based GV being exceeded
· GV at 10-5 lifetime excess cancer risk not feasible
WHO Guidelines for Drinking-Water Quality
|
1983-4 |
Publication of first edition |
|
1993-6 |
Publication of second edition |
|
1997 |
First addendum to second edition |
|
1999 |
Second addendum to second edition |
|
2001 |
Third addendum to second edition |
|
2004 |
Third edition |
Protection and Control of Water Quality
Aim to include balanced, integrated guidance on monitoring and assessment of drinking-water supply and quality and on the elements of risk management in the Guidelines in 2003.
Monitoring and assessment of water supply and quality:
» Volume 3 coverage good for rural areas
» Guidance for urban settings will be developed, field tested and revised
Risk management:
» resource and source protection
» water treatment
» chemicals and materials
» significant expansion
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Microbiological Aspects
Session Objectives
· To highlight the number and range of pathogens that may be found in water.· To describe some of the key preventative and monitoring actions which maintain and improve microbiological water quality.
· To introduce the concept and use of indicator bacteria in water quality monitoring.
· To describe the principal indicator bacteria used and their key characteristics which make them suitable for use as indicators.
· To emphasise the value of E.coli and thermotolerant faecal coliforms as routine indicators.
Summary
The wide variety of waterborne diseases is the most important concern about water quality, and their public health impact has far-reaching implications. The pathogens concerned include many types of viruses, bacteria, protozoa and helminths, which differ widely in size, structure and composition. This implies that their survival in the environment and resistance to water treatment processes differs significantly. However, the waterborne transmission of infectious diseases can be controlled effectively by practical and economic methods. The approach must be based on protection of the source, selection of appropriate treatment methods, fail-safe application of the treatment methods, well protected distribution networks and appropriate quality monitoring. Relatively simple and inexpensive indicator methods are available for routine monitoring of the microbiological safety of water and the efficiency of treatment processes. Most reliable results are obtained by high frequency testing for indicator organisms selected for particular purposes. For instance, routine monitoring programmes for drinking-water may be based on tests for faecal streptococci, thermotolerant coliform organisms or Escherichia coli. Under certain circumstances, tests for the heterotrophic plate count and coliphages may be included. These tests are simple, inexpensive and yield results in a relatively short time. More complicated and expensive tests such as those for human viruses and protozoan parasites are required only for particular purposes, including research and assessment of the efficiency of treatment processes.
1. Introduction
Waterborne diseases are the most important concern about the quality of water. Developing countries and rural communities are particularly vulnerable. In developed countries the mortality due to waterborne diseases is low, but the socio-economic impact is phenomenal (Avendano et al, 1993; Payment, 1993).
Waterborne diseases are typically caused by enteric pathogens which belong to the group of organisms basically transmitted by the faecal-oral route. In other words, they are mainly excreted in faeces by infected individuals, and ingested by others in the form of faecally contaminated water or food. Some of the pathogens may be of animal origin. Some may also be transmitted by personal contact, droplet transfer, or inhalation of contaminated aerosols. Water may also play a role in the transmission of pathogens which are not faecally excreted. These include opportunistic pathogens which are members of the normal flora of the external human body. Some of these pathogens are natural inhabitants of certain water environments. Most waterborne pathogens are distributed world-wide, but outbreaks of some, for instance cholera and hepatitis E, tend to be regional. Dracunculiasis is geographically limited to rural areas in India, Pakistan, and sixteen countries in sub-Saharan Africa.
1.1 Enteric pathogens typically transmitted by the faecal-oral route
|
Bacteria: |
Salmonella spp, Shigella spp, pathogenic Escherichia coli, Campylobacter spp, Vibrio cholerae and Yersinia enterocolitica. |
|
Viruses: |
Hepatitis A and E, enteroviruses, adenoviruses, small round structured viruses including Norwalk virus, astro and rota viruses. |
|
Protozoa: |
Entamoeba histolytica, Giardia intestinalis, Cryptosporidium parvum. |
1.2 Helminths
Infections contracted by exposure to, or ingestion of, infectious larval stages of human parasites released by specific snails or cyclops:
Schistosoma spp (schistosomiasis, bilharziasis) and Dracunculus medinensis (dracunculiasis guinea worm). The latter is not faecally excreted but typically transmitted by water and of major public health importance in some countries.
1.3 Opportunistic pathogens
Infections of the skin and mucous membranes of the eye, ear, nose and throat:
Pseudomonas aeruginosa, Aeromonas, and species of Mycobacterium.
Infections contracted by the inhalation of contaminated aerosols:
Legionella spp (legionellosis), Naegleria fowleri (primary amoebic meningo-encephalitis) and Acanthamoeba spp (amoebic meningitis, pulmonary infections).
1.4 Toxins from cyanobacteria
Toxins released by blooms of cyanobacteria (blue-green algae) such as Microcystis aeruginosa may adversely affect the health of animals and possibly also humans.
1.5 Nuisance organisms
A variety of non-pathogenic micro-organisms, and small plants and animals, may under undesirable conditions thrive in water supplies and cause turbidity, taste and odour, or visible animal life, which are aesthetically objectionable.
Bacterial contamination of drinking-water has resulted in numerous cases of infectious disease. The massive cholera epidemic in Latin America, which spread from Peru to several other countries, and the recent one in Rwanda, are reminders of the speed with which certain waterborne diseases can spread.
Viruses feature prominently among the wide variety of waterborne pathogens. Examples include the 1991 outbreak with 70,000 cases of hepatitis E caused by polluted drinking-water in Kanpur (Grabow et al, 1994a). Reasons for the high incidence of waterborne viral infections include excretion in exceptionally high numbers by infected individuals, relatively high resistance to unfavourable environmental conditions including water treatment and disinfection processes, and a minimal infectious dose which may be as low as a single viable viral particle (Payment, 1993). The impact of viral infections is aggravated by secondary and even tertiary transmission by routes other than the water which caused the original infection (Morens et al, 1979). Epidemiological studies on waterborne viral infections are complicated by the absence of clinical symptoms in many individuals, particularly children, while all infected individuals excrete viruses at similar rates.
Recent years have seen a substantial increase in the number of waterborne Giardia and Cryptosporidium outbreaks. The cysts and oocysts of these protozoan parasites are extremely resistant to water treatment and disinfection processes, and their minimal infectious dose is low (Casemore, 1991; Craun, 1991).
Despite modern technology and know-how, waterborne diseases continue to have a major public health and socio-economic impact, and at least in parts of the world their incidence may even increase (Craun, 1991). Challenges to control waterborne diseases are complicated by continuous changes in the composition and priority of waterborne pathogens. Factors which affect the occurrence of pathogens include changes in population densities, socio-economic situations, standard of living, education, vaccination, climate, geography, urbanisation, migration and travelling, and public health policies.
The role of microbiological analysis is very important in a strategy for the control of waterborne diseases based on appropriate treatment systems, appropriate operation of the treatment systems, and appropriate quality monitoring.
2. Water Treatment and Disinfection Technology
A wide variety of treatment systems and disinfection processes are available to ensure the safety of water supplies. At the low technology and inexpensive end of the range there are methods such as simple sand filtration of water, the addition of household bleach to a bucket of drinking-water, storage of water, the exposure of water to sunlight, or boiling of drinking-water. At the other end of the range there are multiple-barrier treatment trains capable of the direct reclamation of drinking-water from waste water. All of these systems are capable of producing safe water. Consideration of the quality of available raw water sources is an integral part of the selection of appropriate treatment methods. The challenge is to select the appropriate system for each particular situation. Each situation has to be evaluated in its own merit, based on considerations such as the raw water quality, intended use of the water, financial resources, and technological capabilities.
3. Operation of Water Treatment Systems
The wide variety of treatment systems capable of producing safe water mentioned above, are without exception subject to potential breakdown and human failure in operation, supervision and quality surveillance. There is not even an indication that in the foreseeable future we can hope for a practical fail-safe water treatment system. Successful operation and supervision of treatment systems, improvement of technical capabilities, and training programmes aimed at meeting water quality requirements, are very important. The production of safe water is not possible without fail-safe operation and supervision of treatment systems (Bellamy, 1993).
4. Microbiological Water Quality Monitoring
Transmission of diseases by treated water supplies can be ascribed to inappropriate treatment methods, failure in operation and supervision, or shortcomings in quality monitoring. In fact, it can theoretically be argued that all waterborne diseases can be prevented by appropriate monitoring and corrective measures taken in good time. Since there is no indication that we can expect to see practical fail-safe treatment systems, or an elimination of human failure or error in the operation and supervision of treatment systems, appropriate microbiological quality monitoring will remain an indispensable component of strategies for the control of waterborne diseases.
Regular inspection of sanitary and hygienic aspects of raw water sources, treatment facilities and distribution networks is an important component of quality monitoring programmes, and is particularly important with regard to pathogens such as viruses and protozoan parasites which are not readily detectable in water.
4.1 Indicator organisms
Since it would be practically impossible to test water for each of the wide variety of pathogens that may be present, microbiological water quality monitoring is primarily based on tests for indicator organisms. There is no single indicator organism that can universally be used for all purposes of water quality surveillance. Each of the wide variety of indicators available for this purpose has its own advantages and disadvantages, and the challenge is to select the appropriate indicator, or combination of indicators, for each particular purpose of water quality assessment.
Indicators most commonly used are of faecal or sewage origin, and the following are some of the most important requirements of such indicators:
a) Present whenever pathogens are present.b) Present in the same or higher numbers than pathogens.
c) Specific for faecal or sewage pollution.
d) At least as resistant as pathogens to conditions in natural water environments, and water purification and disinfection processes.
e) Non-pathogenic.
f) Detectable by simple, rapid and inexpensive methods.
Ideally, various other properties are desirable, such as counts which are directly related to those of pathogens. However, the fundamental and most important requirement is that pathogens should be absent or inactivated whenever indicators are absent or inactivated.
Many indicators have been studied and recommended for water quality assessment (ISO, 1990; Standard Methods 1992). Evaluation of the reliability of indicators is carried out by comparison of their incidence and survival in water and treatment processes with that of selected pathogens, by epidemiological studies on the consumers of water supplies, by calculations based on the minimal infectious dose of pathogens, and by experiments with human volunteers (Regli et al, 1991). The following is a summary of the most important features of commonly used indicators:
4.1.1 Escherichia coli
This species is a member of the group of faecal coliform bacteria. Escherichia coli has the important feature of being highly specific for the faeces of man and warm-blooded animals. For all practical purposes these bacteria cannot multiply in any natural water environment and they are, therefore, used as specific indicators for faecal pollution. They are generally distinguished from other thermotolerant coliforms by the ability to yield a positive indole test within 24 hours at 44.5°C. More recently, E. coli is also identified by possession of the enzyme �-glucuronidase, which hydrolyses the fluorogenic substrate 4-methyl-umbelliferyl-�-D-glucuronide (MUG) with release of the fluorogen which can be observed in liquid media under ultraviolet light. Media based on hydrolysis of MUG are commercially available under names such as "Colilert". Such complex sets of tests for the final confirmation of E. coli are not recommended as a routine.
4.1.2 Thermotolerant coliform bacteria
This term refers to certain members of the group of total coliform bacteria which are more closely related to faecal or sewage pollution, and which generally do not readily replicate in water environments. This group of bacteria is also known as faecal coliforms, presumptive E. coli, faecal E. coli, faecal coli, etc. Thermotolerant coliforms are primarily used for the assessment of faecal pollution in waste water and raw water sources. They are detectable by simple and inexpensive tests, and are widely used in routine water quality monitoring. The test methods used are the multiple tube and membrane filtration using mFC medium and incubation for 24 hours at 44.5°C. In the membrane filtration individual colonies can be identified, and the presence of Escherichia coli provides strong evidence of faecal pollution.
4.1.3 Coliform bacteria (total coliforms)
The term "coliform bacteria" refers to a vaguely defined group of Gram-negative bacteria which have a long history in water quality assessment. In outdated literature these bacteria go by all sorts of names, including coliforms, colis, etc. Some of the bacteria included in this group are almost conclusively of faecal origin, while other members may also replicate in suitable water environments. These bacteria, which can be determined by simple and inexpensive tests, are primarily used for assessment of the general sanitary quality of finally treated and disinfected drinking-water. Methods used are multiple tube or membrane filtration using LES Endo agar and incubation for 24 hours at 35-37°C. More recently coliform bacteria are also identified by their possession of the enzyme �-D-galactosidase, which hydrolyses chromogenic substrates such as ortho-nitrophenyl-�-D-galactopyranoside (ONPG), resulting in release of the chromogen and a colour change in liquid media.
The primary purpose of coliform tests is not to detect faecal pollution but to screen the general sanitary quality of treated drinking-water supplies.
4.1.4 Enterococci
Enterococci, sometimes referred to as faecal streptococci, is a group of bacteria more closely related to faecal pollution than total coliforms because most members of this group do not replicate as readily in water environments. These Gram-positive bacteria tend to be more resistant than faecal coliforms (Gram-negative), and are detectable by practical techniques, such as membrane filtration using m-enterococcus agar and incubation at 44.5° or 37°C for 48 hours. Presently the group is considered to primarily include only Enterococcus faecalis, E. faecium, E. durans and E. hirae. More recently enterococci are identified by the ability to hydrolyse 4-methyl-umbelliferyl-�-D-glucoside (MUD) in the presence of thallium acetate, nalidixic acid and 2,3,5-triphenyl-2H-tetrazolium chloride (TTC) resulting in release of the fluorogen which in liquid media is readily detectable under ultraviolet light.
4.1.5 Sulphite-reducing clostridia
An important advantage of these Gram-positive anaerobic bacteria is that their spores are more resistant to conditions in water environments, as well as treatment and disinfection processes, than most pathogens, including viruses. Clostridia are sometimes considered as too resistant, and their inclusion in water quality guidelines as too stringent. One of the members of the group, Clostridium perfringens, is like E. coli highly specific for faecal pollution. Clostridia generally occur in lower numbers in waste water than coliform bacteria. Detection methods are relatively expensive and time-consuming.
4.1.6 Heterotrophic plate count
This test is also known as the total or standard plate count. The test detects a wide variety of organisms, primarily bacteria, which give an indication of the general microbiological quality of water. The test is simple and inexpensive, yields results in a relatively short time, and has proved one of the most reliable and sensitive indicators of treatment or disinfection failure. The generally used test method is pour plates using a rich growth medium such as yeast extract agar and incubation for 48 hours at 37°C.
4.1.7 Other indicators
A variety of other indicators has been used in water quality assessment, including cytopathogenic human viruses, Pseudomonas aeruginosa, Staphylococcus aureus, acid-fast bacteria, Legionella species, Candida albicans, and endotoxins. All of these have advantages for certain purposes.
4.2 Protozoan parasites
The cysts and oocysts of intestinal parasites such as Giardia and Cryptosporidium species are exceptionally resistant, and they generally occur in low numbers in raw and treated water supplies (Casemore, 1991; Bellamy et al, 1993). In addition, they are not readily detectable, and their behaviour in water treatment and disinfection processes differs extensively from that of commonly used indicators. Quality control is, therefore, generally based on specifications for raw water quality and the efficiency of treatment processes rather than indicators or testing for cysts and oocysts (Regli et al, 1991).
4.3 Human viruses
The incidence and behaviour of human viruses in water environments and treatment processes may differ extensively from that of faecal indicators for reasons such as:
a) Viruses are excreted only by infected individuals, and coliform bacteria by almost all people and warm-blooded animals. Numbers of viruses in water environments are, therefore, generally lower than those of indicators such as faecal coliforms by several orders of magnitude.b) Viruses are excreted for relatively short periods in numbers of up to 1012/g of faeces, while coliform bacteria are excreted fairly consistently in numbers of about 109/g of faeces.
c) The structure, composition, morphology and size of viruses differs fundamentally from that of bacteria, which implies that behaviour and survival in water differ.
In view of the above differences it is not surprising that bacterial indicators such as coliform bacteria have shortcomings as indicators for viruses. These shortcomings have been confirmed in epidemiological studies and research on the incidence of indicators and viruses in water supplies. Ideally water quality surveillance should, therefore, include tests for viruses. Unfortunately, however, tests for viruses are relatively expensive, complicated and time consuming, and require sophisticated facilities and know-how. In addition, the great majority of viruses concerned are not detectable by conventional virological cell culture techniques. Control of the virological safety of water is, therefore, as in the case of protozoan parasites, often based on raw water quality and specifications for purification and disinfection processes rather than testing of the treated water (Regli et al, 1991).
4.4 New developments in microbiological water quality monitoring
4.4.1 Bacteriophages
Bacteriophages (phages) are viruses which infect bacteria. In terms of size, structure, morphology and composition they closely resemble human viruses. The behaviour of phages in water and related environments, and their resistance to unfavourable conditions, treatment systems and disinfection processes do, therefore, more closely resemble those of human viruses than bacterial indicators of faecal pollution.
Phages can replicate only in specific host bacteria, which implies that the phages of E. coli (coliphages) are, like their hosts, related to faecal pollution. Phages commonly used in water quality assessment include the groups of phages known as somatic and male-specific coliphages, which each have their own indicator advantages and disadvantages. Phages which infect Bacteroides fragilis strain HSP40 are highly specific for human faeces, and can be used to distinguish between faecal pollution of human and animal origin (Grabow et al, 1994b). Evidence supporting the indicator value of phages is accumulating, and their inclusion in quality monitoring protocols is gaining ground rapidly.
4.4.2 Virological analysis of water
Although desirable, virological analysis is not included in many routine surveillance protocols because of cost, complexity and time. In addition, the great majority of viruses concerned are not detectable by conventional techniques. However, progress is being made in the development of more practical and meaningful techniques, and virological monitoring for certain purposes is becoming more feasible. Challenges include the recovery of small numbers of viruses from large volumes of water, the detection of a wider variety of viruses, and reduction in the cost of testing (Standard Methods, 1992).
4.5 Indicator strategies in water quality surveillance
Since no single indicator can fulfil all the needs of water quality surveillance, best results are obtained by using appropriate combinations of indicators for various purposes. Each of these indicators offers certain information, which in combination yields a reliable picture of the quality of the water under investigation. For instance, indicators selected for monitoring the quality of treated drinking-water supplies may primarily be based on tests for Escherichia coli to detect faecal pollution. However, under certain circumstances indicators such as the heterotrophic plate count, total coliforms and somatic coliphages may yield valuable additional information.
Breakdown in treatment plants, and human error in operation and supervision, generally take place without warning, in fact, like a thief at night they tend to strike when least expected. This implies that quality surveillance programmes should make provision for microbiological monitoring at the highest possible frequency, in order to detect problems at the earliest possible stage. Since monitoring programmes are subject to many variables and considerations, including the raw water source and treatment system concerned, as well as available financial resources, facilities and manpower, it is not possible to formulate universal sampling protocols. Each case has to be evaluated in its own merit. With regards to sampling frequencies, it is important to keep in mind that it is better to run simple and inexpensive tests at high frequency than complicated and expensive tests at low frequency.
Important principles in sampling procedures include aseptic collection in sterile containers, and delivery at the laboratory for testing preferably within two hours of collection. The inclusion of samples collected at the consumer's tap is advisable, and so is the collection of samples at different times of the day and different days of the week.
5. Microbiological Water Quality Guidelines
Water quality guidelines and standards recommended by various authorities are similar in that they intend to ensure the minimum risk of infection. However, they differ in detail because of considerations such as economic and technical capabilities, and perceptions of acceptable risks of infection.
The Guidelines state that drinking-water must not contain waterborne pathogens. More specifically, E. coli or thermotolerant coliforms should not be present in 100 ml samples of drinking-water at any time, for any type of water supply, treated or untreated, piped or unpiped. In the case of large supplies, where sufficient numbers of samples are examined, total coliforms are acceptable in the distribution system in a maximum of 5% of samples taken throughout any 12 month period (Annex 1).
If guideline values are exceeded, immediate investigative action must be taken, including repeat testing, and thorough inspection of the treatment plant and its operation, the raw water source, and general hygiene of the water distribution system.
It is recognised that, in the great majority of rural water supplies in developing countries, faecal contamination is widespread and achieving the guideline values for E. coli or thermotolerant coliforms is often not possible. Under these conditions, the national surveillance agency should set medium-term targets for the progressive improvement of water supplies, as recommended in Volume 3 of Guidelines for drinking-water quality (Surveillance and control of community supplies).
Because routine monitoring techniques are not available for viruses, protozoa and helminths of health significance, the Guidelines recommend protection of the source and treatment techniques to ensure their absence. The degree of treatment required is a function of the nature (ground or surface water) and level of faecal contamination of the source.
To ensure the absence of viruses, the Guidelines recommend that the following conditions of disinfection with chlorine be met:
|
Residual free chlorine |
³ |
0.5 mg/litre |
|
Contact time |
³ |
30 minutes |
|
pH |
< |
8.0 |
|
Median turbidity |
£ |
1 Nephelometric Turbidity Unit (NTU) |
|
Maximum turbidity |
= |
5 NTU |
The control of pathogenic protozoa and guinea-worm requires efficient filtration since these organisms are rather resistant to disinfection.
6. Conclusions
· Waterborne diseases have a major public health and socio-economic impact, and are the most important concern of water quality.· Strategies for the control of waterborne diseases must be based on the selection of appropriate water sources and treatment systems, fail-safe operation of these treatment systems, and reliable bacteriological quality monitoring.
· A wide variety of treatment and disinfection systems is available for reliable production of microbiologically safe drinking-water.
· Reliable guidelines for the microbiological safety of drinking-water are available.
References
Avendano P, Matson D O, Long J, Whitney S, Matson C C and Pickering L K (1993). Costs associated with office visits for diarrhea in infants and toddlers. Pediatric Infectious Diseases Journal 12, 897-902.
Bellamy W D, Cleasby J L, Logsdon G S and Allen M J (1993). Assessing treatment plant performance. Journal of the American Water Works Association 85, 34-38.
Casemore D P (1991). The epidemiology of human cryptosporidiosis and the water route of infection. Water Science and Technology 24, 157-164.
Craun G F (1991). Causes of waterborne outbreaks in the United States. Water Science and Technology 24, 17-20.
Grabow W O K, Favorov M O, Khudyakova N S, Taylor M B, and Fields H A (1994a). Hepatitis E seroprevalence in selected individuals in South Africa. Journal of Medical Virology (in press).
Grabow W O K, Neubrech T E, Holtzhausen C S and Jofre J (1994b). Bacteroides fragilis and Escherichia coli bacteriophages: excretion by humans and animals. Water Science and Technology. (Submitted for publication).
ISO (1990). Detection and enumeration of coliform organisms, thermotolerant coliform organisms, and presumptive Escherichia coli.
Part 1: Membrane filtration method (9308-1:1990).
Detection
and enumeration of coliform organisms, thermotolerant coliform organisms, and
presumptive Escherichia coli.
Part 2: Multiple tube (most probable
number) method (9308-2:1990).
Morens D M, Zweighaft R M, Vernon T M, Gary G W, Eslien J J, Wood B T, Holman R C and Dolin R (1979). A waterborne outbreak of gastroenteritis with secondary person-to-person spread: Association with a viral agent. The Lancet i, 964-966.
Payment P (1993). Prevalence of disease, levels and sources. In: Safety of Water Disinfection: Balancing Chemical and Microbial Risks. International Life Sciences Institute, Washington DC.
Regli S, Rose J B, Haas C N and Gerba C P (1991). Modelling the risk from giardia and viruses in drinking-water. Journal of the American Water Works Association 92, 76-84.
Standard Methods (1992). Standard Methods for the Examination of Water and Wastewater, 18th Edition. Eds.: A E, Clesceri L S, Eaton A D. American Public Health Association, Washington DC. pp 9-1 - 9-147.
Annex 1
BACTERIOLOGICAL QUALITY OF
DRINKING-WATER
|
Organisms |
Guideline value |
|
All water intended for drinking | |
|
E. coli or thermotolerant coliform bacteria |
Must not be detectable in any 100-ml sample |
|
Treated water entering the distribution system | |
|
E. coli or thermotolerant coliform bacteria |
Must not be detectable in any 100-ml sample |
|
Total coliform bacteria |
Must not be detectable in any 100-ml sample |
|
Treated water in the distribution system | |
|
E. Coli or thermotolerant coliform bacteria |
Must not be detectable in any 100-ml sample |
|
Total coliform bacteria |
Must not be detectable in any 100-ml sample. In the case of large supplies, where sufficient sample are examined, must not be present in 95% of samples taken throughout any 12-month period. |
Presentation Plan
|
Section |
Key points |
OHP |
|
Introduction |
· very many different types of microorganisms in water, some of which are harmful (pathogens) and some of which are not |
Table 1 & 2 |
| |
· pathogens may be bacteria, viruses or parasites | |
|
Pathogens in water |
· Guidelines considered many types of pathogens including bacteria, viruses, protozoa and helminths |
1 |
| |
· Pathogens have distinguishing properties that make them very different from chemical pollutants and influence GV setting | |
| |
· GV not set for pathogens as there is no lower tolerable limit, any ingestion of pathogens represents some risk to health | |
|
Monitoring and preventative actions |
· water quality is prone to rapid variability and failures often discrete events |
2 |
| |
· water quality failure may be caused by poorly protected sources, inadequate or failures in treatment or leaking distribution systems |
|
|
|
· to ensure water quality need to use four key approaches: water quality analysis, sanitary inspection, source protection & minimum treatment requirements | |
| |
· water quality analysis only identifies contamination once it has occurred, sanitary inspection identifies potential risks and source protection and minimum treatment limit risks |
|
|
The need for indicators |
· analysis of pathogens difficult, expensive and is essentially a reactive process - fails to provide a warning about potential problems |
3 |
| |
· therefore need a system to identify water supplies which represent a health risk before disease outbreaks occur | |
| |
· risks associated with faecal contamination, so use indicator bacteria which indicate faecal contamination | |
|
Properties of indicators |
· faecal indicators should be present in water where there is faecal contamination |
4, 5 |
| |
· indicators should be present in greater numbers than pathogens |
|
|
|
· they should have the same resistance to disinfectants and environmental stress as the most resistant pathogens | |
| |
· they should not multiply under environmental conditions | |
| |
· should be easy and cheap to carry out analysis of indicators |
|
|
Examples of indicators |
· number of indicators may be used |
6 |
| |
· these have different characteristics and may be used for different purposes or under different conditions | |
| |
· examples of indicator bacteria include: total coliforms, thermotolerant coliforms, E.coli, faecal streptococci, Clostridium and Pseudomonas | |
| |
· these all derive purely or in part from human faeces and are present in large numbers | |
| |
· indicator bacteria are not particularly effective in indicating presence of viruses which are more resistant and persistent than bacteria | |
| |
· coliphages may also be used as indicators, although this is under debate at present | |
|
Principal indicator bacteria |
· the most commonly used indicators are total, thermotolerant coliforms and E.coli |
7 |
| |
· total coliforms grow at 37oC, but do not come from a purely faecal origin | |
| |
· presence of total coliforms in water supplies indicates a leakage or biofilm problem and thus a potential risk from ingress of surface water |
|
|
|
· E.coli is the most commonly used faecal indicator bacteria for which thermotolerant (faecal) coliforms are an accepted substitute |
|
|
|
· there should be zero thermotolerant coliforms in 100 ml of drinking water | |
|
The use of other indicators |
· other indicators may be used for other reasons such as indication of operational problems or because they are more resistant to disinfection than coliforms | |
| |
· faecal streptococci are more persistent than E. coli and rarely multiply in polluted water, but may come from animal faeces | |
| |
· however, they tend to be present in lower numbers than E. coli | |
Problems in Setting Guideline Values for Individual Pathogens
· Pathogens are discrete and not in solution· Pathogens often in clumps or adhere to suspended solids
· Cannot predict likelihood of infectious dose from average concentration
· Infection and disease development dependent on invasiveness, virulence and immunity
· Dose-response not cumulative
Ensuring Microbiological Quality
· Water quality analysis
· Sanitary inspection
· Source protection
· Minimum treatment requirements
Need for Faecal Indicator Organisms
· Pathogen analysis:
» expensive
» impracticable
» techniques may be time consuming
» reactive
· Reliance is therefore placed on relatively simple and more rapid tests for the detection of certain intestinal bacteria which indicate that faecal contamination could be present.
Characteristics of the Ideal Faecal Indicator
1. Should be present in wastewater and contaminated water when there are pathogens2. Should be present when there is a risk of contamination by pathogens
3. Should be present in greater numbers than the pathogens
4. Should not multiply in environmental conditions under which pathogens cannot multiply
5. The indicator population should correlate with the degree of faecal contamination.
6. The survival time in unfavourable environmental conditions should exceed that of pathogens
7. Should be more resistant to disinfectants and other stresses than the pathogens
8. Should present no health risk
9. Should be easy to enumerate and identify by simple methods
10. Should have stable characteristics and give consistent reactions in these analyses
Examples of Indicator Organisms
| |
Percentage in mammal faeces |
LOG10/g | |
|
Total coliforms |
Viable, but many environmental sources | | |
|
Thermotolerant coliforms |
100 (environmental source in tropical waters?) |
7-9 | |
|
E. coli |
100 |
7-9 | |
|
Faecal streptococci |
100 |
5-6 | |
|
Clostridium perfringens |
13-35 |
6-7 | |
|
Pseudomonas aeruginosa |
3-15 |
3-5 | |
|
Bacteriodes fragilis |
100 |
7-10 | |
|
Coliphages |
| | |
| |
· Somatic |
60 |
1-8 |
| |
· F-Specific |
6 |
1-2 |
Principal Indicator Bacteria
Principal indicator bacteria are:
· Escherichia coli
· Faecal coliforms (95% are E.coli, ± 44oC)
· Faecal streptococci
Table 1: Examples of Pathogens Considered in the Guidelines
|
Pathogen |
Health significance |
Persistence in water supplies |
Resitance to chlorine |
Relative infectious dose |
Important animal reservoir |
|
Bacteria | |||||
|
Camplyobacter jejuni, C.coli |
High |
Moderate |
Low |
Moderate |
Yes |
|
Pathogenic E.coli |
High |
Moderate |
Low |
High |
Yes |
|
Salmonella typhi |
High |
Moderate |
Low |
High |
No |
|
Shigella spp. |
High |
Short |
Low |
High |
No |
|
Vibrio cholera |
High |
Short |
Low |
High |
No |
|
Yersina enterocolitica |
High |
Long |
Low |
High (?) |
Yes |
|
Pseudomonas aeruginosa |
Moderate |
May multiply |
Moderate |
High (?) |
No |
|
Aeromonas spp. |
Moderate |
May multiply |
Low |
High (?) |
No |
|
Viruses | |||||
|
Adenoviruses |
High |
? |
Moderate |
Low |
No |
|
Enterovirus |
High |
Long |
Moderate |
Low |
No |
|
Hepatitus A |
High |
? |
Moderate |
Low |
No |
|
Norwalk virus |
High |
? |
? |
Low |
No |
|
Rotavirus |
High |
? |
? |
Moderate |
No (?) |
|
Small round virus |
Moderate |
? |
? |
Low (?) |
No |
|
Protozoa | |||||
|
Entamoeba histolytica |
High |
Moderate |
High |
Low |
No |
|
Giardia intestinalis |
High |
Moderate |
High |
Low |
Yes |
|
Cryptosporidium parvum |
High |
Long |
High |
Low |
Yes |
|
Helminths | |||||
|
Dracunulus medinensis |
High |
Moderate |
Moderate |
Low |
Yes |
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Disinfectants and Disinfection By-Products
Session Objectives
· To describe the importance of disinfection in providing safe drinking water.· To describe the key disinfectants evaluated in the Guidelines and describe their principal characteristics and effectiveness.
· To describe the key by-products formed by the principal disinfectants and describe the likely health risk from their presence in water.
· To describe the balance between microbiological and chemical health risks and emphasise the need to prioritise microbiological quality.
Introduction
Disinfection of drinking-water is essential if we are to protect the public from outbreaks of waterborne infectious and parasitic diseases. The main disinfectants evaluated in the Guidelines are free chlorine, chloramines, chlorine dioxide and ozone.
As much as the perfect indicator organism does not exist, each of the commonly used disinfectants has its advantages and disadvantages in terms of cost, efficacy, stability, ease of application and formation of by-products.
Table 1 summarizes the Ct values for the four main disinfectant,
where
C = disinfectant concentration in mg/litre, and
t = the contact time in minutes required to inactivate a specified percentage of microorganisms.
Table 1: Summary of C.t values (mg/L. min)for 99% inactivation at 5°C (Clark et al, 1993)
|
Organism |
Disinfectant | |||
| |
Free chlorine, pH 6 to 7 |
Pre-formed chloramine, pH 8 to 9 |
Chlorine dioxide, pH 6 to 7 |
Ozone, pH 6 to 7 |
|
E. coli |
0.034-0.05 |
95-180 |
0.4-0.75 |
0.02 |
|
Polio virus 1 |
1.1-2.5 |
768-3740 |
0.2-6.7 |
0.1-0.2 |
|
Rotavirus |
0.01-0.05 |
3806-6476 |
0.2-2.1 |
0.006-0.06 |
|
Bacteriophage f2 |
0.08-0.18 |
- |
- |
- |
|
G. lamblia cysts |
47->150 |
- |
- |
0.5-0.6 |
|
G. muris cysts |
30-630 |
- |
7.2-18.5 |
1.8-2.0a |
|
C. parvum |
7200b |
7200c |
78b |
5-10c |
a Values for 99.9% inactivation at pH 6-9.
b 99% inactivation at pH 7 and 25°C.
c 90% inactivation at pH 7 and 25°C.
From the Ct values, ozone is the most efficient and chloramine the least efficient, particularly for viral agents. Free chlorine is more effective than chlorine dioxide with regard to E. coli and rotavirus. Chlorine dioxide is more effective than free chlorine with regard to the protozoa Giardia lamblia and muris. Ozone is the most efficient disinfectant for cryptosporidium parvum. As the temperature increases, the Ct values decrease for all disinfectants. The effect of pH varies with the nature of the disinfectant and is most pronounced for chlorine.
Chlorine and its by-products
Chlorine is the most widely used drinking-water disinfectant. When added to water the following reaction occurs within a second or less:
Cl2 + H2O = HOCl + H+ + Cl-
The magnitude of the equilibrium hydrolysis constant is such that hydrolysis to hypochlorous acid, HOCl, is virtually complete in fresh water at pH > 4 and at chlorine doses up to 100 mg/litre (Morris, 1982).
Hypochlorous acid is a weak acid that dissociates partially in water as follows:
HOCl = H+ + OCl-
The value of the acid ionization constant is about 3 × 10-8. As shown in Figure 1, at 20°C and pH 7.5, there is an equal distribution of HOCl and OCl-. At pH 8, about 30% of the free chlorine is present as HOCl, and at pH 6.5, 90% is present as HOCl (Morris, 1982). The term free chlorine refers to the sum of hypochlorous acid and hypochlorite ion. Since HOCl is a considerably more efficient disinfectant than OCl-, and free chlorine, even as hypochlorite, is more effective than combined chlorine (e.g. chloramines), the Guidelines recommend that disinfection be carried out at pH less than 8 and at a free chlorine concentration ³ 0.5 mg/litre.
Of all the disinfectants, the chemistry and toxicity of the reaction by-products of chlorine have been the most extensively studied.
Figure 1: Distribution of
hypochlorous acid and hypochlorite ion in water at different pH values and
temperatures (Morris, 1951)
Since Rook's discovery of the formation of haloforms during chlorination of Rotterdam water supply (Rook, 1974), numerous halogenated compounds have been identified in chlorinated drinking-water and their toxicity assessed. Precursors of these halogenated compounds include natural humic and fulvic compounds and algal material. The most commonly found chlorine disinfection by-products are the trihalomethanes (THM), halogenated acetic acids, halogenated acetonitriles, chloral hydrate and the chlorinated phenols. Others include chlorinated furanone MX, halopicrins, cyanogen halides, haloketones and haloaldehydes. The halogenated disinfection by-products identified account for only about half of the total formed.
Based on animal toxicological studies, Guideline Values (GVs) have been recommended for a number of these compounds. Undoubtedly, the third edition of the Guidelines, planned for the year 2002, will include additional chlorination by-products.
The following chemicals resulting from chlorination of water supplies have been evaluated in the Guidelines:
· free chlorine (HOCl + OCl-)
· trihalomethanes
· chlorinated acetic acids
· halogenated acetonitriles
· chloral hydrate (trichloroacetaldehyde)
· chlorophenols
· MX (3-chloro-4-dichloromethyl-5-hydroxy-2(5H)-furanone)
For countries wishing to control DBP, it may not be necessary to set standards for all of the DBP for which guideline values have been proposed. The trihalomethanes, of which chloroform is the major component, are likely to be the main DBP, together with the chlorinated acetic acids in some instances. In many cases, control of chloroform levels and, where appropriate, trichloroacetic acid will also provide an adequate measure of control over other chlorination by-products.
(a) Chlorine
Free chlorine in drinking-water is not particularly toxic to humans. The major source of exposure to chlorine is drinking-water. Therefore, 100% of the TDI was allocated to drinking-water giving a health-based GV of 5 mg/litre for the sum of hypochlorous acid and hypochlorite ion. Based on the taste and odour threshold of free chlorine, it is doubtful however that consumers would tolerate such a high level of chlorine. Most individuals are able to taste chlorine at concentrations below 5mg/litre, and some at levels as low as 0.3 mg/litre. The health-based GV for chlorine should not be interpreted as a desirable level of chlorination.
(b) Trihalomethanes
The predominant chlorine disinfection by-products are the THMs. Nevertheless, they account for only about 10% of the total organic halogen compounds formed by water chlorination.
THMs are formed by the aqueous chlorination of humic substances, of soluble compounds secreted from algae and of naturally occurring nitrogenous compounds (Morris, 1982). THMs consist primarily of chloroform, bromodichloromethane, dibromochloromethane and bromoform.
When bromide is present in drinking-water, it is oxidized to hypobromous acid by chlorine:
HOCl + Br- = HOBr + Cl-
HOBr reacts with natural organic compounds to form brominated halomethanes. Similarly, the presence of iodide may lead to the formation of mixed chlorobromoiodo-methanes.
Some generalized statements can be made with regard to THMs in chlorinated drinking-water (IARC, 1991; Morris, 1982; Canada, 1993):
· Concentration of THMs in drinking-water varies widely and ranges from not detectable to 1 mg/litre or more;· THM levels are higher in chlorinated surface water than in chlorinated groundwater;
· Concentrations of THMs tend to increase with increasing temperature, pH and chlorine dosage;
· Concentrations of THMs increase upon storage even after exhaustion of residual chlorine or after dechlorination. This indicates the formation of intermediates products leading to the slow production of THMs;
· Chloroform is usually the most abundant THM often accounting for greater than 90% of the total THM concentration;
· If there is a significant amount of bromide in the raw water, the brominated THMs, including bromoform, may be dominant;
· Formation of THMs can be minimized by avoiding pre-chlorination and by effective coagulation, sedimentation and filtration to remove organic precursors prior to final disinfection;
· Removal of THMs after their formation is difficult and involves resource-intensive processes such as activated carbon adsorption or air stripping.
Because trihalomethanes usually occur together, it has been the practice to consider total trihalomethanes as a group, and a number of countries have set guidelines or standards on this basis, ranging from 0.025 to 0.25 mg/litre.
In the 1993 WHO Guidelines, individual GV have been recommended for the four trihalomethanes. With an underlying assumption that the THMs may exert potential toxic effects through similar biological mechanisms, authorities may want to establish standards for total THMs that would account for possible additive effects and not simply add up the guideline values for the individual compounds in order to arrive at a standard. Instead, the following approach is recommended:

where
C = concentration, and
GV = guideline value
Epidemiological studies of carcinogenicity of chlorine and DBP
In 1991, WHO International Agency for Research on Cancer (IARC) published an evaluation of the carcinogenic risks to humans of chlorinated drinking-water based on a number of animal toxicological and epidemiological studies. IARC concluded that because of one or more methodological weaknesses, the epidemiological studies reviewed cannot constitute the basis of valid risk assessment.
The epidemiological investigation of the relation between exposure to chlorinated drinking-water and cancer occurrence was considered problematic because any increase in relative risk over that in people drinking unchlorinated water is likely to be small and therefore difficult to detect in epidemiological studies. In all of the studies evaluated, estimates of exposure were imprecise and surrogates (e.g surface versus groundwater) do not reflect exposure during the relevant time periods for the etiology of the cancers in question. Many variables, such as smoking habits, dietary practices, use of alcohol, socio-economic status, and ethnicity are known to affect cancer incidence and were not taken into account in most of the studies (IARC, 1991).
In its overall evaluation, IARC concluded that there is inadequate evidence for the carcinogenicity of chlorinated drinking-water in humans as well as in experimental animals (IARC, 1991).
Chloramine and its by-products
Chloramine generally produces by-products similar to those observed with chlorine but at much lower concentrations. An exception to this is the formation of cyanogen chloride, CNCl (Bull and Kopfler, 1991). The use of chloramine as a disinfectant has increased in recent years because of limited formation of THMs, however, little is known about the nature of other byproducts.
Monochloramine is about 2000 and 100 000 times less effective than free chlorine for the inactivation of E. coli and rotaviruses, respectively. Monochloramine cannot therefore be relied upon as primary disinfectant. It is useful for maintaining a residual disinfectant in distribution systems. The shift to monochloramine to control THM formation may thus compromise disinfection and the Guidelines caution against such procedure. Organic chloramines are even less effective disinfectants than monochloramine.
Chlorine dioxide and its by-products
Because of its explosive hazard, chlorine dioxide is manufactured at the point of use. CLO2 is generated through the reaction of sodium chlorite and chlorine. Chlorine dioxide reactions with humic substances do not form significant levels of THMs. In addition, it does not react with ammonia to form chloramines. The main disinfection by-products of chlorine dioxide are chloride, chlorate and chlorite.
Chlorine dioxide is more effective towards inactivation of Giardia cysts than free chlorine, but less effective towards rotavirus and E. coli. Unlike chlorine, the disinfection efficiency of chlorine dioxide is independent of pH and the presence of ammonia.
A provisional GV was recommended for chlorite while no adequate data were available to recommend a GV for chlorate. No GV has been recommended for chlorine dioxide per se because of its rapid breakdown in aqueous solutions and the chlorite GV is adequately protective for potential toxicity from chlorine dioxide. Furthermore, the taste and odour threshold for chlorine dioxide in water is 0.4 mg/litre which constitutes a limiting factor and a signal for its presence at higher concentrations in drinking-water.
Other reaction by-products of chlorine dioxide with organics in drinking-water have not been well characterized but include aldehydes, carboxylic acids, haloacids, chlorophenols, quinones and benzoquinone (Bull and Kopfler, 1991). In a recent article, more than 40 organic disinfection by-products were identified in a pilot plant in Indiana which uses chlorine dioxide as a primary disinfectant. The toxicity of these by-products is largely unknown (Richardson et al. 1994).
Ozone and its by-products
Ozone decomposes rapidly following application, and for this reason no GV has been proposed for ozone.
By products of ozonation that have been identified include formaldehyde and other aldehydes, carboxylic acids, hydrogen peroxide, bromate, bromomethanes, brominated acetic acids, brominated acetonitriles and ketones. Guideline values have been recommended for bromate and formaldehyde.
Ozone is the most efficient disinfectant for all types of microorganisms. Disadvantages include lack of disinfectant residual, biological regrowth problems in distribution systems, high cost, and limited information on the nature and toxicity of its by-products.
Balancing Chemical and Microbial Risks
Quantitative assessments of risks associated with the microbial contamination of drinking-water are scarce. Although there are gaps in our knowledge, we cannot afford to postpone action until rigorous quantitative assessment of chemical versus microbial risks are available and every answer is known.
A semi-quantitative presentation of risks associated with disinfection was first attempted by Morris (1978) and is given in Figure 2. The following is more or less a quote of his work: The risk of waterborne infectious disease is very high when no chlorination is used, and drops sharply to a low value when even minimal levels of chlorination are maintained. We know this on the basis of a century's experience, Morris stated. As the level of chlorination is increased the risk continues to drop slightly, but never quite reaches zero, for no system is perfect. At very high levels of chlorine the microbial risk increases as taste and odour may cause the use of unsafe supplies.
Figure 2: Risks and benefits of
water chlorination (Morris, 1978)
The chemical risk does not start at zero for there is some hazard connected with the organic matter before chlorination. The chemical risk decreases initially because destruction of chemicals by oxidation more than compensate for the formation of new chemicals at low levels of chlorination. Because of the formation of by-products, the chemical risk increases with increasing level of chlorination. Intuitively, he depicted the chemical risk from chlorination as being considerably lower than the microbial risk from a non-disinfected supply.
In developed countries, since filtration and chlorination became common for community water supplies, morbidity and mortality due to waterborne intestinal diseases, particularly typhoid fever and cholera, have declined to negligible levels. Almost all of the waterborne outbreaks that still occur are associated with the use of untreated water or water from systems in which chlorination was inadequate.
Other health impact studies concern the beneficial effects on health of safe and sufficient water supplies and adequate sanitation, three factors that are so intertwined that it is often not feasible to draw definite lines of demarcations between them. Together, they constitute the pillars of public health protection. Projected reduction in morbidity achievable through the provision of safe and sufficient water supplies and adequate sanitation are estimated to be (WHO, 1992):
|
|
Projected reduction in morbidity (%) |
|
Cholera, typhoid |
80 |
|
Diarrhoeal diseases |
40 |
|
Dracunculiasis |
100 |
|
Schistosomiasis |
60 |
When applying these percentage reductions to the global morbidity and mortality rates for these diseases, the benefits of saving millions of lives through these interventions are immediately apparent.
As shown in Figure 3 overleaf, provision of safe drinking-water can result in a 20% reduction in infant mortality (Regli et al., 1993).
In their pioneering work on comparison of estimated risk from known pathogens in untreated surface water and chlorination by products in drinking-water, Regli et al. (1993) concluded that:
· the risk of death from pathogens is at least 100 to 1000 times greater than the risk of cancer from disinfection by-products (DBPs);· the risk of illness from pathogens is at least 10 000 to 1 million times greater than the risk of cancer from DBPs;
· morbidity and mortality rates from pathogens compared with those from DBPs, may be considerably higher in developing countries where the sanitary and health status is not as good;
· in societies where infant mortality and life expectancy is low, many people would not be expected to live long enough to incur cancer, which also causes much higher differences in risk resulting from exposure to pathogens versus DBPs cited above.
While this last statement seems cynical, it does reflect the true situation in many developing countries.
Figure 3: Infant mortality versus
access to safe water (Regli et. al., 1993)
Conclusion
Adequate disinfection of drinking-water is the most important priority to assure a safe water supply. Recent cholera outbreaks in Latin America and Rwanda provide dramatic evidence of the importance of adequate water disinfection. There is some limited evidence of possible health effects from disinfectant by-products, particularly possible cancer risks from chloroform and the other trihalomethanes and by-products. This evidence is based on high-dose animal studies.
Epidemiological studies conducted to date do not provide any evidence that disinfectants and their by-products affect human health at the concentrations found in drinking-water. The International Agency for Research on Cancer has concluded that there is inadequate evidence for the carcinogenicity of chlorinated drinking-water in humans and experimental animals.
Although stated in qualitative way, the message of the Guidelines is clear:
The estimated risks to health from disinfectants and their by-products are extremely small in comparison to the real risks associated with inadequate disinfection, and it is important that disinfection should not be compromised in attempting to control such by-products. The destruction of microbial pathogens through the use of disinfectants is essential for the protection of public health.
All disinfectants by necessity are reactive substances and produce by-products. Little is known about the nature and toxicity of the by-products of ozone, chlorine dioxide or chloramines. The by-products of chlorination are the ones that have been most extensively identified and their toxicity assessed. Disinfection with chlorine should not be penalized for this reason. In addition, in many countries, if disinfection can be practised at all, it will be through the use of chlorine.
There are now more and more indication that the estimated risks to health from disinfectants and their by-products are several order of magnitude lower than the real risks associated with inadequate disinfection. So while there is great scientific certainty that inadequately disinfected water results in devastating microbial disease epidemics, there is relatively great uncertainty regarding the possible health risks from DDBPs. In establishing standards for disinfectants by products, it is emphasized that "Where local circumstances require that a choice must be made between meeting either microbiological guidelines or guidelines for disinfectants or disinfectant by-products, the microbiological quality must always take precedence, and where necessary, a chemical guideline value can be adopted at a higher level of risk. Efficient disinfection must never be compromised." (1993 Guidelines)
References
Bull R.J., Kopfler F.C. (1991). Health Effects of Disinfectants and Disinfection By-products, American Water Works Association, Denver.
Canada Health and Welfare (1993). Water treatment principles and applications. Canadian water and wastewater association, Ottawa.
Clark RM, Hurst CJ, Regli S (1993). Costs and benefits of pathogen control in drinking-water. In: Safety of water disinfection: balancing chemical and microbial risks. Craun G.F. ed. ILSI Press, Washington, D.C.
International Agency for Research on Cancer (1991). IARC monographs on the evaluation of carcinogenic risks to humans, Volume 52 Chlorinated drinking-water; chlorination by-products; some other halogenated compounds; cobalt and cobalt compounds, Lyon.
Morris J.C. (1951), unpublished research, Harvard University, 1951
Morris J.C. (1978). Conference summary. In: Water chlorination environmental impact and health effects. Volume 2. Jolley RL, Gorchev H., Hamilton D.H. eds., Ann Arbor Science, Ann Arbor, Michigan.
Morris J.C. (1982). Health perspective in the oxidative treatment of water for potable supply. Part 2 Health assessment of current oxidant-disinfectants. National Institute for Water Supply. Leidschendam, Netherlands.
Regli S., Berger P., Macler B., Haas C. (1993). Proposed decision tree for management of risks in drinking-water: consideration for health and socioeconomic factors. In: Safety of water disinfection: balancing chemical and microbial risks. Craun G.F. ed. ILSI Press, Washington, D.C.
Richardson S.D., Thruston A.D., Collette T.W. (1994). Multispectral identification of chlorine dioxide disinfection byproducts in drinking-water. Environ. Sci. Technol., 28: 592-599.
Rook J.J. (1974). Formation of haloforms during chlorination of natural waters. J. Soc. for water treatment and examination 23: 234-243.
World Health Organization (1992). Our planet, our health. Report of the WHO Commission on health and environment. Geneva.
Annex 1
BACTERIOLOGICAL QUALITY OF
DRINKING-WATER
|
Organisms |
Guideline value |
|
All water intended for drinking | |
|
E. coli or thermotolerant coliform bacteria |
Must not be detectable in any 100-ml sample |
|
Treated water entering the distribution system | |
|
E. coli or thermotolerant coliform bacteria |
Must not be detectable in any 100-ml sample |
|
Total coliform bacteria |
Must not be detectable in any 100-ml sample |
|
Treated water in the distribution system | |
|
E. Coli or thermotolerant coliform bacteria |
Must not be detectable in any 100-ml sample |
|
Total coliform bacteria |
Must not be detectable in any 100-ml sample. In the case of large supplies, where sufficient sample are examined, must not be present in 95% of samples taken throughout any 12-month period. |
Table 1: Summary of C.t values (mg/L. min) for 99% inactivation at 5°C (Clark et al, 1993)
|
Organism |
Disinfectant | |||
| |
Free chlorine, pH 6 to 7 |
Pre-formed chloramine, pH 8 to 9 |
Chlorine dioxide, pH 6 to 7 |
Ozone, pH 6 to 7 |
|
E. coli |
0.034-0.05 |
95-180 |
0.4-0.75 |
0.02 |
|
Polio virus 1 |
1.1-2.5 |
768-3740 |
0.2-6.7 |
0.1-0.2 |
|
Rotavirus |
0.01-0.05 |
3806-6476 |
0.2-2.1 |
0.006-0.06 |
|
Bacteriophage f2 |
0.08-0.18 |
- |
- |
- |
|
G. lamblia cysts |
47->150 |
- |
- |
0.5-0.6 |
|
G. muris cysts |
30-630 |
- |
7.2-18.5 |
1.8-2.0a |
|
C. parvum |
7200b |
7200c |
78b |
5-10c |
a Values for 99.9% inactivation at pH 6-9.
b 99% inactivation at pH 7 and 25°C.
c 90% inactivation at pH 7 and 25°C.
Presentation Plan
|
Section |
Key points |
OHP |
|
Introduction |
· disinfection of all waters supplied for drinking is recommended by WHO to protect public health |
1,2 |
| |
· main disinfectants evaluated in the Guidelines are: free chlorine, chloramines, chlorine dioxide and ozone | |
| |
· overall ozone is the most effective disinfectant, although chlorine is also effective and efficient |
|
| |
· all disinfectants have advantages and disadvantages and all produce by-products | |
| |
· a number of disinfection by-products were evaluated in the GDWQ | |
|
Chlorine and its by-products |
· chlorine is most common disinfectant |
3,4,5 |
| |
· when chlorine is added to water it forms hypochlorous acid, hydrogen ion and a chlorine ion | |
| |
· because of greater efficiency, the Guidelines recommend disinfection with chlorine is done at pH less than 8 and a free chlorine concentration of greater than 0.5 mg/l | |
| |
· the use of chlorine leads to the formation of halogenated by-products, including the THMs | |
| |
· precursors to THMs are natural humic and fulvic acids and algal material | |
| |
· numerous other by-products may be formed (see paper or Guidelines for examples) | |
| |
· impurities in gaseous and liquid chlorine of relevance to the nature of by-products are carbon tetrachloride and bromide | |
| |
· GVs set for a number of chlorination by-products | |
| |
· very difficult to estimate exposure to halogenated organic compounds in drinking-water | |
| |
· may not need to set standards for all by-products included in Guidelines, it is better to concentrate on the major groups(e.g. THMs) |
|
|
|
· microbiological quality of water should never be compromised by concerns about disinfection by-products | |
|
Chlorine |
· free chlorine in drinking-water is not particularly toxic and health-based GV is 5 mg/l | |
| |
· very unlikely consumers would accept such levels of chlorine as taste is noted as low as 0.3 mg/l | |
| |
· do not use GV as desirable level of chlorination | |
|
Tri-halomethanes |
· these are principal by-products of chlorination, but only form 10 per cent of total organic compounds in drinking-water |
6 |
| |
· THMs more likely to occur in chlorinated surface water than groundwater | |
| |
· THM concentrations vary widely; increasing with increasing temperature, pH, chlorine dosage and on storage after exhaustion of free chlorine or dechlorination | |
| |
· chloroform is most common THM (usually >90% of total THMs) |
|
|
|
· when bromine present, brominated THMs likely to be dominant | |
| |
· THM formation can be minimised by avoiding prechlorination and by optimising treatment | |
| |
· THM removal is expensive and difficult | |
|
Chloramine and by-products |
· chloramines formed by reaction of chlorine and ammonia or organic amines |
7 |
| |
· can get mono-, di- and trichloramines depending on pH and temperature | |
| |
· chloramine by-products similar to free chlorine, with exception of cyanogen chloride | |
| |
· monochloramine about 2000 to 100, 000 times less effective than free chlorine for inactivation of E.coli and rotaviruses |
|
|
Chlorine dioxide and by-products |
· chlorine dioxide made at point of use because of its explosive hazard |
8 |
| |
· chlorine dioxide does not form THMs or chloramines | |
| |
· main by-products are chlorite, chlorate and chloride | |
| |
· chlorine dioxide more effective than free chlorine in inactivation of Giardia cysts but less effective against E.coli and rotaviruses | |
| |
· no GV for chlorine dioxide in water as it rapidly disassociates |
|
|
|
· GVs set for chlorite but not for chlorate | |
|
Ozone and by-products |
· ozone decomposes rapidly following application and thus no GV has been proposed |
9 |
| |
· by-products include formaldehyde, other aldehydes, hydrogen peroxide and bromomethanes (see paper/Guidelines for further examples) | |
| |
· ozone is the most efficient disinfectant with regard to microorganisms | |
| |
· disadvantages include: lack of residual, biological regrowth problems in distribution systems, high cost and limited information on nature and toxicity of by-products | |
| |
· when ozonation followed by chlorination, concentrations of brominated THMs may increase | |
|
Balancing chemical and microbial risks |
· currently a scarcity of quantitative assessment done of relative risks of microbial and chemical contamination of drinking-water |
10 |
| |
· semi-quantitative presentation has been done by Morris: this showed that risk of infectious water-borne disease is high where chlorination not practised and this decreases sharply with even minimal levels of chlorination, though can never reach zero risk | |
| |
· at very high chlorine concentrations, microbial risk increases as taste and odour cause the use of unsafe supplies | |
| |
· chemical risks do not start at zero as always some hazard from organic matter prior to chlorination | |
| |
· chemical risks are low initially but increase with increasing chlorine dosages | |
| |
· risk of death from pathogens is at least 100 to 1000 times greater than risk of cancer from disinfected by-products and risk of illness from pathogens at least 10,000 to 1 million times greater | |
| |
· morbidity and mortality rates from pathogens compared to cancer risk from by-products may be much higher in developing countries where sanitary and health status poor | |
|
Conclusions |
· disinfection is important to assure a safe drinking-water supply |
|
|
|
· limited information is available concerning health risk from disinfection by-products | |
| |
· disinfection by-product formation may be reduced if treatment process are optimised and prechlorination is avoided | |
| |
· inadequate evidence exists concerning the carcinogenicity of chlorinated drinking-water | |
| |
· more information is available concerning chlorine because it has been studied in more detail and this should not penalise the use of chlorine |
|
|
|
· as microbiological quality is of paramount importance, disinfection should not be compromised | |
Disinfectants Evaluated
· Chlorine
· Chloramine
· Chlorine dioxide
· Ozone
· Iodine
Disinfectants and Disinfectant by-products
· Overall ozone is the most effective disinfectant, although chlorine is effective and efficient· All disinfectants have advantages and disadvantages and all produce by-products
· A number of disinfectant by-products were evaluated in the Guidelines
Microbiological quality of water should never be compromised by concerns about disinfection by-products

Distribution of Hypochlorous Acid
and Hypochlorite Ion in Water at Different pH Values and Temperatures

Relationship between Measured Free
Residual Available Chlorine (HOCl+, OCl-) and
Bactericidally Active (HOCl)
Chlorine
· Chlorine is the most common disinfectant· Chlorine by-products
» Free chlorine
» Trihalomethanes (THMs)
» Chlorinated acetics acids
» Halogenated acetonitriles
» Chloral hydrate (trichloroacetaldehyde)
» Chlorophenols
» MX
(3-chloro-dichlormethyl-5-hydroxy-2(5H)-furanone)
May not need to set standards for all by-products included in the Guidelines, it is better to concentrate on the major groups (e.g. THMs)
Trihalomethanes
· The principal by-product of chlorination· Formed by the aqueous chlorination of humic substances
· More likely to occur in chlorinated surface water than groundwater
· Concentrations of THMs tend to increase with increaseing temperature, pH and chlroine dosage
· THMs consist primarily of:
» Chlroform
» Bromodichloromethane
» Dibromochloromethane
» Bromoform
· Formation of THMs can be minimised by avoiding prechlorination and optimising treatment
Chloramine and its By-products
· Chloramines formed by reaction of chlorine and ammonia or organic amines· Mono-, di- and trichloramines may be formed depending upon pH and temperature
· Chloramine by-products similar to free chlorine with the exception of cyanogen chloride
· Mono-chloramine is a less effective disinfectant than free chlorine and cannot be relied upon as a primary disinfectant; though useful for maintaining a residual.
Chlorine dioxide and its By-products
· Chlorine dioxide made at point of use because of its explosive hazard· Reactions with humic substances do not form significant levels of THMs or chloramines
· Main by-products are:
» chlorite
» chlorate
» chloride
· More effective than free chlorine in inactivation of Giardia cysts but less effective against E.coli and rotaviruses· No GV for chlorine dioxide in water as it dissociates rapidly. GVs set for chlorite but not chlorate
Ozone and its By-products
· Most efficient disinfectant for all types of micro-organisims· Decomposes rapidly following application thus no GV has been proposed for ozone
· By-products include:
» formaldehyde
» aldehydes
» hydrogen peroxide
» bromomethanes
· Disdavantges include:
» lack of residual
» biological regrowth in distribution systems
» high cost
» limited information on toxicity of its by-products

Balancing chemical and
microbiological
risks
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Inorganic Constituents and Aesthetic Parameters
Session Objectives
· To describe the process of setting Guideline Values for inorganic parameters and describe the narrow divide between toxic and essential elements.· To describe some basic physico-chemical characteristics of water.
· To provide some examples of inorganic chemicals to illustrate the uses of GVs for inorganics and highlight priority substances.
· To describe the basis of monitoring of physical and chemical parameters.
All substances are poisons; there is none which is not a poison. The right dose differentiates a poison and a remedy.
PARACELSUS (1493-1541)
Introduction
Many of the inorganic and aesthetic constituents evaluated in the Guidelines are known to be essential for life. Chromium, copper, fluoride, iodine, manganese, molybdenum, and selenium are essential elements in human nutrition; arsenic and nickel are considered by some researchers as essential elements. Of the aesthetic constituents, iron, chloride, calcium and magnesium (hardness), sodium and zinc are essential elements.
A classification into "essential" and "toxic" elements is fraught with difficulties since as science advances, there is a constant shift of the elements from one group to the other. Toxicity is inherent in all elements, and is a function of the concentration to which humans are exposed. Paracelsus' statement remains valid, "The right dose differentiates a poison and a remedy". Ordinary salt, calcium, magnesium and iron, are all toxic above certain doses. This is illustrated in Figure 1 below.
The plateau of "safe and adequate intake of essential elements" are mainly a matter for nutritionists to decide.

Figure 1. Dose-response curve
(Source: Galal-Gorchev, 1995)
Notes: NOAEL: no observed adverse effect limit; LOAEL: lowest observed adverse effect limit; Threshold chemicals: only toxic above certain dose, therefore have a NOAEL; Non-threshold chemical: toxic at any dose, therefore do not have a NOAEL
No attempt has been made in the Guidelines to define a minimum desirable concentration of essential elements in drinking-water. The Guidelines are concerned with the quantification of toxic effects.
A few of the inorganic chemicals and aesthetic constituents of common interest to many countries will be discussed here to illustrate the approach taken in deriving, or not deriving, guideline values (GV). A complete list of inorganic substances for which GVs have been derived is given in Table A2.2 (A) in Annex 2 of Volume 1 of the Guidelines.
Inorganic Constituents
Asbestos in drinking-water: no health hazard
Because of numerous inquiries from governments, industry and academia on the potential adverse health effects from asbestos in drinking-water, WHO issued the attached Press Release.
Asbestos is used in a large number of applications, particularly construction materials, such as asbestos cement (A/C) sheet and pipe, electrical and thermal insulation, and friction products, such as brake linings.
Asbestos is introduced into water by the natural dissolution of asbestos-containing minerals as well as from industrial effluents, atmospheric pollution, and A/C pipes in water distribution systems. High levels of asbestos have been found in drinking-water from corrosion of A/C pipes.
The asbestos content of food has not been well studied because of the lack of a simple, reliable analytical method. Based on crude estimates, intake of asbestos in food may be significant compared with that in drinking-water. Concentrations of 7 million fibres per litre (MFL) in beer and 12 MFL in soft drinks have been reported.
Asbestos is a known human carcinogen by the inhalation route. Based on the inhalation route, IARC has assigned it to Group 1 (the agent is carcinogenic to humans), while recognising that asbestos behaved differently by the oral route.
Asbestos was not found to be carcinogenic in several animal feeding studies. Epidemiological studies of population exposed to high levels of asbestos in drinking-water (200 MFL) did not reveal any excess cancer risk. It was therefore concluded that ingested asbestos is not hazardous to health and there was no need to establish a GV for asbestos in drinking-water.
Another question that needs to be answered is: Can high concentration of asbestos fibres in drinking-water become airborne and create a health hazard?
In a study in New York State, asbestos contamination in excess of 10 billion fibres per litre was detected in a community's drinking-water. Mean airborne asbestos concentrations were significantly higher in a small number of homes with water containing this elevated concentration of asbestos than in three control homes; however, the difference in concentrations was primarily due to increased numbers of short (<1 µm) fibres, which are considered to contribute little to health risk. Moreover, all fibre concentrations determined in this limited study were within the range of those measured in indoor and outdoor air in other investigations.
In another study, using a conventional drum-type humidifier, testing showed that release of asbestos fibres to air from water containing 40 ± 10 MFL was negligible.
The final question - does corrosive water transported in A/C pipe pose any specific or unique health risk? Corrosive water does not create a specific health risk as it relates to A/C pipe since asbestos fibres in drinking-water do not pose a health risk and are not transferred into the air. However, corrosive water is an important problem that must be addressed by all water utilities no matter what type of water pipe material is used in the distribution system or homes. Proper selection of the quality of A/C pipes is important and some national institutions have issued standards for A/C pipes suitable for water with different degrees of aggressiveness.
Fluoride and dental health
Fluoride levels between 0.5 and 1 mg/litre provide substantial protection against dental caries. However, for fluoride, the margin between beneficial and toxic effects is rather small (see Figure 1). Excessive exposure may lead to adverse health effects varying from mottling of teeth to crippling skeletal fluorosis.
The Guidelines recommend a GV of 1.5 mg/litre on the assumption that the daily per capita consumption of drinking-water is about 2 litres. At this level, dental fluorosis may occur in a certain proportion of the population. In setting national standards for fluoride, it is particularly important to consider climatic conditions, volumes of water intake, and intake of fluoride from other sources (e.g. food, air).
Nitrate and nitrite
Nitrate and nitrite in drinking-water may be of natural origin, or can be leached from septic tanks, pig farms and feed lots. Use of fertilizers (too much and at the wrong time of the year) can also result in nitrate pollution.
High concentration of nitrate, and especially nitrite in drinking-water may cause methaemoglobinaemia. Groups especially susceptible to methaemoglobin formation are young infants, children and pregnant women.
Epidemiological studies indicate that at levels of nitrates less than 50 mg/litre (as nitrate), there does not seem to be any problem with methaemoglobinaemia. There are considerable uncertainties as to the level of nitrite which may cause such clinical effects. On the assumption that nitrite was ten times more potent than nitrate (on a molar basis) with respect to methaemoglobin formation, the Guidelines recommend a provisional GV of 3 mg/litre (as nitrite). In addition, since nitrite and nitrate exert similar toxicological effect and may occur simultaneously, the following condition was also specified:
where
C = concentration in drinking-water
GV = guideline value
Lead and IQ
In 1986 the Joint FAO/WHO Expert Committee on food Additives (JEFCA) established a provisional tolerable weekly intake (PTWI) of lead from all sources of 25 µg lead/kg body weight (equivalent to 3.5 µg/kg body weight per day) for infants and children on the basis that lead is a cumulative poison and that there should be no accumulation of body burden of lead. In 1993, the Committee reconfirmed this PTWI and extended it to all age groups.
Assuming a 50% allocation of the PTWI to drinking-water for a 5-kg bottle-fed infant consuming 0.75 litres of drinking-water per day, the health-based guideline value is 0.01 mg/litre (rounded figure).
The most significant health effect from lead is the association of lead exposure with reduced cognitive development and intellectual performance in children. Results of studies on children with blood lead concentrations below 25 µg/dl indicate that, on average, the intelligence quotient (IQ) is reduced by 1-3 points for each 10 µg/dl increment in the blood lead concentration. Existing epidemiological studies do not provide evidence of a threshold.
Steps are now being taken to reduce all sources of lead exposure of children with some apparent success in various countries. In countries where lead has been removed from petrol, and where there is no specific source of excess lead exposure, blood lead concentrations in children are decreasing and are now approximately 4-6 µg/dl. The almost complete elimination of lead-soldered side-seams in canned foods in a number of countries has also contributed to the reduction in lead exposure. Corrosion control measures are being implemented to reduce the lead content of drinking-water and new plumbing and fittings now seldom contain lead.
Aesthetic Aspects
Contrary to the 1984 Guidelines, the 1993 Guidelines do not propose guideline values for substances and parameters that affect the acceptability of drinking-water to consumers. The Review Groups were of the opinion that guideline values should be recommended only for those substances that are directly relevant to health. A list of substances which may give rise to consumer complaints is given in Table A2.5 in Volume 1 of the Guidelines.
In the case of characteristics based on human sensory evaluation, judgement is often subjective. Aesthetic/organoleptic characteristics are very much subject to social, economic and cultural considerations, and the establishment of standards for the aesthetic quality of drinking-water should take into consideration implementation possibilities, and the existing socio-economic and environmental constraints. When resources are severely limited, establishment of priorities becomes even more important, and such priorities should be set in relation to their direct impact on health. Some countries have elected to set enforceable standards for constituents of health significance, whereas recommendations only are made for aesthetic and organoleptic characteristics.
Total dissolved solids
Total dissolved solids (TDS) in drinking-water consist mainly of chloride, sulphate, carbonates, sodium, magnesium and calcium. Excessive dissolved solids in drinking-water may lead to objectionable taste, and corrosion or encrustation in water distribution system. At concentrations greater than approximately 1000 mg/litre, the taste of water becomes increasingly unpalatable.
As far as health aspects are concerned, there is no evidence of adverse physiological reactions at TDS levels greater than 1000 mg/litre. On the contrary, there are vague indications from epidemiological studies that high levels of certain salts (calcium and magnesium) may have beneficial health effects.
It should be emphasized that the factor of acclimatization to TDS is particularly important. Many people enjoy highly mineralized waters containing more than 2000 mg/l of TDS.
Removal of TDS from drinking-water is an expensive proposition, and if a national standard for TDS is being considered, it should take into account the feasibility of implementation.
Turbidity
Particles in drinking-water are aesthetically objectionable, and can serve as shields for pathogenic microorganisms. Moreover, many toxic chemicals such as pesticides and heavy metals are selectively adsorbed on suspended particulate matter. The efficiency of disinfection may be reduced in the presence of turbidity: the disinfectant is unable to reach the target organism because of a physical barrier and/or chemical reactions with turbidity particles may occur thus decreasing the available disinfectant concentration. Where disinfection is practised, the turbidity should preferably be less than 1 Nephelometric Turbidity Unit and always below 5.
The effect of turbidity depends on its physico-chemical characteristics. Certain water supplies, such as groundwater, may contain non-organic turbidity, which may not affect disinfection. The complex factors involved in the potential health risk from the presence of turbidity precluded the derivation of a health-based GV.
References
WHO (1994) Fluorides and oral health. WHO Technical Report Series 846. Geneva.
WHO (1993) Evaluation of certain food additives and contaminants (lead). WHO Technical Report Series 837. Geneva.
Presentation Plan
|
Section |
Key points |
OHP |
|
Introduction |
· many of both the inorganic substances and aesthetic parameters evaluated in the Guidelines are known to be essential for life |
1,2 |
| |
· classification of substances into 'toxic' and 'essential' is fraught with difficulties. With ongoing research there is a constant shift of substances between the two groups | |
| |
· toxicity is inherent in all substances, the dose or concentration of a substance differentiates between a poison and a remedy | |
| |
· safe and adequate intake and concentrations for essential substances is a matter for nutritionists | |
| |
· Guidelines do not define a minimum desirable concentration of essential elements, they only define toxic levels | |
|
Physico-chemical characteristics of water |
· water has set of physico-chemical characteristics which affect quality in their own right and influences the ability of water to contain other substances |
3,4 |
| |
· physical characteristics include: temperature, colour, turbidity, suspended solids and dissolved solids | |
| |
· chemical characteristics include: pH, alkalinity, acidity, hardness, dissolved oxygen and oxygen demand | |
|
Asbestos |
· asbestos is widely used and may be a reinforcement in concrete |
|
|
|
· asbestos in water has been shown to have no adverse health effect | |
| |
· asbestos pipes should be protected from 'aggressive' water |
|
|
Fluoride |
· margin between toxic and essential levels is very narrow |
5 |
| |
· fluoride levels between 0.5mg/l & 1mg/l protect against dental caries | |
| |
· exposure to excess levels of fluoride may give rise to adverse health effects from mottling of teeth to crippling skeletal fluorosis |
|
|
|
· GV set at 1.5 mg/l on basis of consumption of 2 litres per day, above this dental fluorosis expected in some of population | |
|
Nitrate & nitrite |
· may be of natural origin or leached from on-site sanitation, intensive animal husbandry, also from inappropriately applied fertiliser |
6 |
| |
· high nitrate and nitrite concentrations may lead to methaemoglobinaemia in infants and pregnant women | |
| |
· GV of 50mg/l nitrate set, as below this epidemiological studies indicate that there is no significant risk of methaemoglobinaemia | |
| |
· uncertainty concerning concentration of nitrite that leads to clinical effects, assumed 10 times more potent than nitrate, GV of 3 mg/l given | |
| |
· as both may occur together, important that the sum of the ratio of concentration of nitrite to the GV and concentration of nitrate to the GV is £ 1 |
|
|
Lead |
· exposure to excess lead may lead to intellectual impairment in children |
7 |
| |
· no threshold for health effects have been identified |
|
|
|
· all exposure to lead is now being reduced and in the water supply this means removal of lead pipes and lead-containing fittings. | |
|
Aesthetic aspects |
· no GVs set for these in the 2nd edition as these are highly societal influenced | |
| |
· turbidity should be kept to below 1TU as above this level disinfection may be compromised, although in some groundwaters have non-organic turbidity which does not affect disinfection |
|
Introduction
"All substances are poisons; there is none which is not a poison. The right dose differentiates a poison and a remedy".
Paracelsus (1493-1541)
Dose-response of Chemicals
Source: Galal-Gorchev, 1995
Physical Characteristics of Water
· Temperature
· Taste and odour
· Colour
· Turbidity
· Suspended solids
· Conductivity
· Total dissolved solids
Chemical Characteristics of Water
· pH
· Alkalinity
· Acidity
· Hardness
· Dissolved oxygen
· Oxygen demand
· Nitrogen
· Chloride

Sources of Fluoride and Impact on
Health
Guideline Value for Nitrate and Nitrite in Drinking-water
where:
C = concentration
GV = Guideline Value
Lead and
Health
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Organic Chemicals
Session Objectives
· To demonstrate the range of organic chemicals that may be found in drinking-water and describe the sources of such chemicals.· To describe the health risks associated with the consumption of drinking-water containing organic contaminants.
· To highlight the taste and odour problems associated with organic contamination.
Introduction
Specific chlorinated alkanes, chlorinated ethylenes, aromatic hydrocarbons, chlorinated benzenes, and miscellaneous organic chemicals were evaluated in the 1993 WHO Guidelines for Drinking-Water Quality.
Many of these organic chemicals are widely used as solvents, in chemical synthesis, in petroleum products, and in the production of plastics and resins. Some 30 organic chemicals were evaluated and guideline values (GV), or provisional guideline values, recommended for 27 of these.
Some organic substances do not have a 'no observed adverse effect limit' (NOAEL) - the highest concentration of a substance which causes no detectable adverse health effect. Therefore for some substances, a provisional guideline has been set on the basis of the 'lowest adverse effect limit' (LOAEL) - the lowest concentration or dose of a substance where there is a detectable adverse effect. Where a LOAEL is used, an additional uncertainty factor (UF) - a measure of the uncertainty regarding the information about a substance - is used. For further information, please refer to the background paper for Session II of this teaching pack or to the Guidelines Volume 1 and 2.
Adequate toxicological data were not available to derive guideline values for a number of chemicals, including 1,1-dichloroethane, 1,3-dichlorobenzene, dialkyltins, and a number of polynuclear aromatic hydrocarbons, with the exception of benzo[a]pyrene.
For most of the aromatic hydrocarbons and chlorinated benzenes, the taste and/or odour thresholds of these chemicals are well below the health-based guideline values, thus constituting an assurance that the GVs would not be exceeded or even approached. Consumers complaints would constitute a safety net against such a situation.
A number of organic chemicals were considered to be genotoxic and carcinogenic and the linearized multistage extrapolation model was used to derive guideline values corresponding to an upper bound estimate of an excess cancer risk of 10-5.
For most organic chemicals that show a threshold for toxic effects, little was known of the magnitude of exposure from drinking-water relative to other sources. Consequently, the default value of 10% of the TDI was allocated to drinking-water.
Nitrilotriacetic acid (NTA) is a compound used in detergents, and tributyltin oxide (TBTA) is used in boat paints. Substantial exposure may occur from drinking-water, and consequently 50% and 20% of the TDI was allocated to drinking-water for NTA and TBTA respectively.
Di(2-ethylhexyl)adipate and di(2-ethylhexyl)phtalate are used in food-contact materials and therefore exposure from food is expected to be high. Therefore, only 1% of their respective TDI was allocated to drinking-water.
Because of their general persistence in the environment and concern over their potential toxicity, a large number of the organic chemicals evaluated are chlorine-containing chemicals.
For further information please see the Guidelines for Drinking Water Quality Volumes 1 and 2.
Presentation Plan
|
Section |
Key points |
OHP |
|
Introduction |
· there are many organic chemicals that may be found in drinking water |
1,2,3 |
| |
· these are very diverse in nature | |
| |
· many organic chemicals found in water are derived from industry |
|
|
The Guidelines |
· the Guidelines review some specific organic chemicals |
4 |
| |
· a total of 30 organic substances reviewed and Guideline derived for 27 of these (inadequate data on the others) | |
|
Exposure from drinking-water |
· for most organics, there is little information available on exposure from drinking-water relative to other sources, therefore have high uncertainty factors | |
| |
· often use a LOAEL rather than a NOAEL as many non-threshold organic subsatnces | |
|
Genotoxic & carcinogenic organics |
· some organics are considered genotoxic and carcinogenic | |
| |
· linerized multistage extrapolation model used to derive GVs corresponding to 10-5 excess risk | |
| |
· most aromatic hydrocarbons and chlorinated benzenes have taste and odour thresholds well below health-based Guideline Values, a margin of safety therefore exists | |
Example of Organic Pollutants by Class and Typical Use 1
· Halogenated aliphatic (chain) hydrocarbons
» Trihalomethanes (THMs) may be formed during disinfection of drinking-water; other compounds used as solvents for decaffeinating coffee, general solvents and in products such as propellant, degreasers, spot removers and dyes
· Aromatic (ring) hydrocarbons
» Many products derived from fossil fuels, also as additives in petrol, moth balls, adhesives and cigarette smoke
· Chloro-and nitro-aromatic hydrocarbons
» Fungicides and explosives
· Phthalates
» Phthalates are added to plastic to make them flexible; found in rain wear, footwear, shower curtains, childrens toys
Example of Organic Pollutants by Class and Typical Use 2
· Halogenated ethers
» Halogenated ethers are used in production of plastics and resins and in research laboratories
· Phenols
» Fungicide; wood preservative; Chloro-dichloro-, trichloro-phenols are by-products in the production of pentachlorophenol
· Organochlorines
» DDT, lindane, aldrin and chlorodane are examples of the extremely persistent organochlorine pesticides widely used in the 1950s and 1960s.
The Breakdown of Organic Compounds
· Enter water from a variety of sources including:
» Human/animal wastes
» Plants
» Soil erosion
» Industrial wastes
· Generally unstable, may be oxidised to stable and relatively inert end products e.g. CO2, NO3, H2O· Oxidation: loss of electrons to an oxidising agent such as oxygen or chlorine which accepts electrons
· Oxidation of organic compounds occurs in aerobic or anaerobic conditions
· Quantity of organic material and the quantity of oxygen needed to oxidise it estimated by using:» Biochemical oxygen demand (BOD)
» Permanganate value (PV)
» Chemical oxygen demand (COD)
Organics reviewed in the Guidelines
· A total of 30 organic substances reviewed in the following groups:
» Chlorinated alkanes (5 substances)
» Chlorinated ethenes (5 substances)
» Aromatic hydrocarbons (6 substances)
» Chlorinated benzenes (5 substances)
» Miscellaneous organic constituents (9 substances)
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Pesticides in Drinking-Water
Session Objectives
· To demonstrate the conflict in pesticide use between agricultural and public health needs.· To describe the two principal methods of pesticide classification.
· To describe the GVs set for pesticides and their by-products.
Pesticides are used for agricultural as well as public health purposes. Often a choice has to be made between their detrimental effects on the environment and their use for disease vector control, as for example, for malaria or schistosomiasis control. The adverse environmental effects of pesticides used in public health can often be mitigated through proper selection and application procedures. Equally, many pesticides have both beneficial and harmful health effects - their use may reduce the presence of particular vectors, although they may be toxic is consumed through water. In these circumstances, the relative benefits and dis-benefits should be evaluated.
With all pesticides, whether they have harmful health effects or not, the application should be well focused both in terms of application technique, quantity used and timing of application. As a general rule, the minimum of pesticide should be applied by the most efficient method at the most suitable time to achive the required goal. Over-application and/or application at times when the action is less likely to be effective should be avoided.
Pesticides can be classified according to chemical class (e.g. organochlorine, carbamate, organophosphorus, chlorophenoxy compounds) or according to their intended use (e.g. fungicide, herbicide, fumigant). It is important to know both since the chemical structure of the pesticide and its use often determine its behaviour in the environment, occurrence in drinking-water and toxicity to humans. Table 1 indicates the chemical class and use of the pesticides evaluated in the Guidelines.
Of the 36 pesticides evaluated, 28 contain chlorine. Organophosphorus pesticides were not evaluated although their use has increased as replacement for organochlorine pesticides. However, the organophosphorus pesticides are readily hydrolysed in water, adsorbed on sediments, or readily degraded in soil. As a result, they are seldom if ever found in drinking-water.
Many of the pesticides evaluated are herbicides. Because of their frequent use near waterbodies they have often been found in surface water. Furthermore many of these herbicides are fairly mobile in soil and readily migrate into groundwater.
While the use of organochlorine pesticides has declined in industrialized countries, their use continues in developing countries for public health as well as for agricultural purposes. For this reason, several organochlorine pesticides were evaluated in the Guidelines.
The toxicological basis of the guideline values and exposure assumptions made, as reflected in the percentage allocation of the TDI to drinking-water, are summarized in Tables 2 and 3.
For organochlorine pesticides such as aldrin/dieldrin, chlordane, DDT, heptachlor, and hexachlorobenzene only 1% of the TDI was allocated to drinking-water since it is known that these pesticides are highly persistent, have a high bioaccumulation potential, and are often found in food (Table 2).
In the majority of cases limited information was available on the contribution of drinking-water to the total exposure. Therefore a default value of 10% of the TDI was used (Table 3).
While considerable information is available on the toxicity of metabolites of pesticides formed in mammalian systems, the nature and toxicity of the environmental degradation products of pesticides are largely unknown and have not been taken into consideration in the Guidelines.
Alachlor, 1,2-dibromo-3-chloropropane, 1,3-dichloropropene and hexachlorobenzene were considered to be carcinogenic. The linearized multistage extrapolation model was therefore used to derive guideline values corresponding to an upper-bound estimate of an excess lifetime cancer risk of 1 per 100,000 of the population exposed.
Because limited information was available on the toxicity of 1,3-dichloropropane, ethylene dibromide and MCPB, no guideline values were derived for these pesticides.
Not all pesticides that have been found in water have been evaluated in the Guidelines. However, over 240 pesticides have been evaluated by the Joint FAO/WHO Meeting on Pesticide Residues (JMPR). Such evaluations could be used by countries wishing to establish standards or guidelines for pesticides of national concern.
In many circumatances, it may not be the principla component of the pesticide which is of concern, but impurities and by-products. It may be more effective to control the release of toxic substances into the aqautic environment through proper product quality control that by establishing standards for drinking-water. It may be more appropriate therefore, to ensure that product quality standards and their enforcement are in place than drinking-water quality standards.
References
International Programme on Chemical Safety (IPCS). Summary of Toxicological Evaluations Performed by the Joint FAO/WHO Meeting on Pesticide Residues, 1996.
Table 1: Chemical family and use of pesticides evaluated in the Guidelines
|
PESTICIDE |
CHEMICAL FAMILY |
USE |
|
alachlor |
CA |
HB |
|
aldicarb |
CB |
AC IN NE |
|
aldrin/dieldrin |
OC |
IN TE |
|
atrazine |
TR |
HB |
|
bentazone |
BT |
HB |
|
carbofuran |
CB |
AC IN NE |
|
chlordane |
OC |
IN TE |
|
chlorotoluron |
UR |
HB |
|
DDT |
OC |
IN |
|
1,2-dibromo-3-chloropropane |
HH |
FM NE |
|
2,4-D |
PO |
HB |
|
2,4-DB |
PO |
HB |
|
1,2-dichloropropane |
HH |
FM |
|
1,3-dichloropropane |
HH |
-- |
|
1,3-dichloropropene |
HH |
FM FU IN NE |
|
dichlorprop |
PO |
HB IG |
|
ethylene dibromide |
BR |
IN FU |
|
fenoprop |
PO |
HB |
|
heptachlor and heptachlor epoxide |
OC |
IN TE |
|
hexachlorobenzene |
OC |
FU |
|
isoproturon |
UR |
HB |
|
lindane |
OC |
IN |
|
MCPA |
PO |
HB |
|
MCPB |
PO |
HB |
|
mecoprop |
PO |
HB |
|
methoxychlor |
OC |
IN |
|
metolachlor |
AM |
HB |
|
molinate |
TC |
HB |
|
pendimethaline |
DA |
HB |
|
pentachlorophenol |
OC |
FU HB IN |
|
permethrin |
PY |
IN |
|
propanil |
AN |
HB |
|
pyridate |
PA |
HB |
|
simazine |
TR |
HB |
|
2,4,5-T |
PO |
HB |
|
trifluralin |
DA |
HB |
Key for Table 1:
Codes for chemical use
|
AM |
acetamide |
|
AN |
anilide |
|
BR |
bromide |
|
BT |
benzothiadiazole |
|
CA |
chloroacetanilide |
|
CB |
carbamate |
|
DA |
dinitroaniline |
|
HH |
halogenated hydrocarbon |
|
OC |
organochlorine |
|
PA |
pyridazine |
|
PO |
phenoxy |
|
PY |
pyrethroid |
|
TC |
thiocarbamate |
|
TR |
triazine |
|
UR |
urea |
Codes for use
|
AC |
acaricide |
|
FM |
fumigant |
|
FU |
fungicide |
|
HB |
herbicide |
|
IG |
growth regulator |
|
IN |
insecticide |
|
NE |
nematicide |
|
TE |
termiticide |
Table 2: Risk assessment of pesticides where substantial exposure from food is expected
|
PESTICIDE |
NOAEL |
UF |
% TDI |
GV, µg/l |
|
aldrin/dieldrin |
0.025 |
250 |
1 |
0.03 (3) |
|
bentazone |
10 |
100 |
1 |
30 |
|
chlordane |
0.05 |
100 |
1 |
0.2 (2B) |
|
DDT |
0.25 |
10 |
1 |
2 (2B) |
|
heptachlor + epoxide |
0.025 |
200 |
1 |
0.03 (2B) |
|
lindane |
0.5 |
100 |
1 |
2 (2B) |
|
permethrin |
5 |
100 |
1 |
20 (3) |
Key:
|
GV |
guideline value |
|
LOAEL |
lowest-observed-adverse-effect level |
|
NOAEL |
no-observed-adverse-effect level |
|
P |
provisional |
|
% TDI |
percent of tolerable daily intake allocated to drinking-water |
|
UF |
uncertainty factor |
Table 3: Risk assessment of pesticides where knowledge of exposure from different media is limited
|
PESTICIDE |
NOAEL |
UF |
% TDI |
GV, µg/l |
|
aldicarb |
0.4 |
100 |
10 |
10 (3) |
|
atrazine |
0.5 |
1000 |
10 |
2 (2B) |
|
carbofuran |
0.05 |
30 |
10 |
5 |
|
chlorotoluron |
11.3 |
1000 |
10 |
30 |
|
2,4-D |
1 |
100 |
10 |
30 (2B) |
|
2,4-DB |
3 |
100 |
10 |
90 (2B) |
|
1,2-dichloropropane |
100 (LOAEL) |
10000 |
10 |
20 P (3) |
|
dichlorpop |
3.64 |
100 |
10 |
100 (2B) |
|
fenoprop |
0.9 |
300 |
10 |
9 (2B) |
|
isoproturon |
3 |
1000 |
10 |
9 |
|
MCPA |
0.15 |
300 |
10 |
2 (2B) |
|
mecoprop |
1 |
300 |
10 |
10 (2B) |
|
methoxychlor |
5 |
1000 |
10 |
20 (3) |
|
metolachlor |
3.5 |
1000 |
10 |
10 |
|
molinate |
0.2 |
100 |
10 |
6 |
|
pendimethalin |
5 (LOAEL) |
1000 |
10 |
20 |
|
pentachlorophenol |
3 |
1000 |
10 |
9 P (2B) |
|
propanil |
5 |
1000 |
10 |
20 |
|
pyridate |
3.5 |
100 |
10 |
100 |
|
simazine |
0.52 |
1000 |
10 |
2 (3) |
|
2,4,5-T |
3 |
1000 |
10 |
9 (2B) |
|
trifluraline |
0.75 |
100 |
10 |
20 (3) |
Key:
|
GV |
guideline value |
|
LOAEL |
lowest-observed-adverse-effect level |
|
NOAEL |
no-observed-adverse-effect level |
|
P |
provisional |
|
% TDI |
percent of tolerable daily intake allocated to drinking-water |
|
UF |
uncertainty factor |
Presentation Plan
|
Section |
Key points |
OHP |
|
Introduction |
· there are conflicting uses of pesticides - agricultural and public health uses | |
| |
· adverse environmental effect of pesicides can often be mitigated through proper selection and application procedures | |
|
Classification |
· there are two methods of
classifying pesticides |
Table 1 |
| |
· it is important to know both these to determine its behaviour in the environment, occurrence in drinking water and toxicity to humans |
|
|
The Guidelines |
· of the 35 pesticides evaluated, 28 contain chlorine |
Tables 2,3 |
| |
· many of the evaluated pesticides are herbicides and readily migrate into groundwater | |
| |
· in developing countries organochlorine pesticides have particular use in public health as well as agricultural practices and have thus been evaluated in the Guidelines | |
| |
· setting GVs for pesticides is often difficult because of uncertaintity about health impacts | |
| |
· the percentage allocation of the TDI to drinking water, reflects the toxicological basis of the Guideline levels and exposure assumptions made |
|
|
|
· the nature and toxicity of the environmental degradation products of pesicides are largely unknown and are therefore not taken into account in the Guidelines | |
| |
· the linearized multistage extrapolation model was used to derive guideline values based on an upper-bound estimate of an excess lifetime cancer risk of 1 per 100,000 of the population exposed | |
| |
· standards and guidelines for pesicides can be established using the evaluations made by the Joint FAO/WHO Meeting on Pesticide Residues |
|
Pesticides in the Guidelines
· Of the 35 pesticides evaluated, 28 contain chlorine· Many of the pesticides evaluated are herbicides and readily migrate into groundwater
· Organochlorine pesticides have been included since they still have public health uses in developing countries
· Setting GVs is difficult due to uncertainty of health impacts
· 10% of the TDI allocated to drinking-water
· Nature and toxicity of the environmental degration products of pesticides are largely unknown
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Monitoring and Assessment of Microbiological Quality
Session Objectives
· To describe the process of planning monitoring and surveillance activities and the need for progression through a number of stages starting with a pilot phase.· To describe the development of analytical ranges in water quality monitoring.
· To introduce the critical parameters concept and emphasise the need for monitoring to focus on health related parameters of water quality.
· To describe the design of sampling networks and frequencies of sampling in routine monitoring programmes.
· To discuss the linkage of monitoring to water supply improvement.
Introduction
The routine monitoring and assessment of the microbiological quality of water is the key priority for both water suppliers and surveillance agencies. Microbiological quality is of principal concern because of the acute risk to health posed by viruses, bacteria and helminths in drinking-water. Therefore, monitoring and assessment of drinking-water is primarily a health-based activity which emphasises the protection of public health through ensuring that the water supplied is of a good quality.
Because monitoring is a health-based activity, other parameters of water supply should also be assessed: quantity, continuity, coverage and cost. All these parameters will affect public health. The water supplier should aim to monitor all aspects of water supply within their area of responsibility and aim for a continuous water supply which is of sufficient quantity and quality at an affordable cost to be available to all the population connected to the supply. The surveillance body should monitor the entire population and identify unserved groups and actively promote universal access to adequate water supplies.
Strategies for monitoring of microbiological quality of safe water should also include hazard identification and risk assessment, processes commonly incorporated within sanitary inspection. It is important that these are systematic and quantifiable and can be used to facilitate decision making at local, regional and national levels on preventative and remedial actions. In addition, minimum treatment requirements and source protection should be emphasised as essential complementary activities to monitoring and assessment.
Planning monitoring and assessment
Monitoring water supply quality will only be effective and efficient if it is properly planned and implemented. In many countries where there has not been routine surveillance and surveillance programmes being developed there may be uncertainty as to what standards should be adopted, the number of water supplies that should be covered, how many samples should be taken, what should be analysed, frequency of inspection etc. These may vary with time and it is important that the surveillance programme remains flexible and open to modification in response to evolving water quality priorities.
In many cases, WHO guideline values are adopted initially as the national standards for drinking-water quality. However, with time these may be superseded by national or regional standards depending on water quality priorities.
When designing a surveillance programme and planning its implementation, it is important that achievable aims and objectives are set. It is useful to clarify these terms: aims are general expression of targets, the 'end' result which is desired, are not generally time constrained. Objectives are indicators of the rate of success in achieving the aim and are specific goals set with definite time scales with indicators of achievement to provide a means of measuring success.
Extensive use of indicator bacteria will be required to monitor microbiological quality and the relative merits of these are discussed in the background paper on the microbiological aspects of water quality and in the Guidelines Volume 1. Thermotolerant (faecal) coliforms are the indicator most widely used for routine monitoring of water quality, although extensive use is also made of total coliforms. In addition to indicator monitoring, routine monitoring of turbidity and chlorine residual (in chlorinated supplies) is recommended in order to ensure that any deterioration of water quality post treatment is rapidly identified.
The rest of this paper will discuss the development of strategies for water quality monitoring and assessment with specific reference to microbiological risks.
Aims and objectives
The aim of surveillance has been defined in Guidelines for drinking-water quality. Volume III (2nd edition) as follows: "Surveillance is an investigative activity which is undertaken in order to identify and evaluate factors associated with drinking-water quality which could pose a risk to health. Surveillance contributes to the protection of public health by promoting the improvement of water supply with respect to quality, quantity, coverage, cost and continuity". Guidelines Volume III also defines the aim of quality control in the water supply sector (which may be seen as an integral part of surveillance) as being: "to ensure that water services meet national standards and institutional targets."
In order to achieve these aims, a number of objectives may be identified, for example:
· the formulation of working methodologies for information gathering, decision making and communication;· the review of existing quality standards and modifications of these as appropriate;
· the identification of appropriate analytical techniques;
· the identification of appropriate equipment and facilities (including evaluation of the use of on-site equipment) required to conduct a surveillance programme;
· identification of analytical quality control procedures for laboratories and on-site techniques and the identification of national (and possibly regional) analytical reference centres;
· establishing staff requirements and assessing skills of current employees, identification of training needs for staff, recruitment needs for the sector;
· to establish a protocol for approval of water sources as fit for drinking;
· to establish whether there are any particular problems in terms of sources, treatment technology, designs, operation and maintenance regimes etc. which are leading to persistent contamination problems.
The time in which it is expected to achieve these objectives must be outlined and indicators selected to measure progress, for instance definition of appropriate chemical assay equipment or type of on-site equipment required.
Routine monitoring of water supplies
In many circumstances, there is a desire to attempt to apply all aspects of surveillance to all the water supplies immediately. Whilst this is a laudable ideal, it is rarely possible to achieve successfully and may lead to resources being over-stretched and the failure of surveillance to provide the expected improvements in water supply quality. This may in turn lead to disappointment and increasing apathy towards surveillance.
Surveillance should be introduced progressively and at each stage objectives set which are achievable and which positively promote the continued development of surveillance. The experience from earlier stages should be used to improve surveillance and lead to a progressively more efficient and comprehensive surveillance programme. Thus, in the initial stages of surveillance, activities may be restricted to sanitary inspections and critical parameter analysis on a restricted number of water supplies. As the programme develops, the number of water supplies covered will be increased, frequency of sampling and inspections increased and the analytical range increased.
Sanitary inspections can be carried out relatively cheaply and easily and can be implemented on all water supplies from the start of surveillance. Sanitary inspection is as much a tool for the supplier or community as the surveillance agency for determining state of the water supply infrastructure and the identification of actual or potential faults and should be carried out on a regular basis by the supplier. The surveillance agency should conduct some independent inspections to verify the reliability of the supplier's information but this does not need to be as frequent.
In the long-term it is desirable that all water supplies should be included in a surveillance programme. However, it is important to be realistic in planning initial surveillance activities taking into account infrastructure, available trained personnel, the number of water supplies in the country and the ability to fund on-going surveillance activities.
Initial surveillance activities may be limited. However, it is important that short, medium and long tern achievable aims and objectives are included in the planning stage of surveillance. There should also be a set of clearly defined indicators that can be used to assess whether targets have been met. The establishment of credible indicators of a monitoring and evaluation programme at the start of the planning process is central to good planning of implementation. Time scales should be attached to each objective and aim and a proposed strategy for achieving these outlined.
Planned surveillance activities will only be possible if there are funds to pay for them and budgets for surveillance require careful preparation. In most cases, there are limited funds available and this inevitably will affect how many supplies can be included, how often they can be visited and how many samples can be analysed. It is therefore imperative that the following are identified and the cost calculated: the number and location of water supplies to be included in each stage of surveillance; staff time; consumable requirements; equipment purchase and maintenance costs; fuel costs; the cost of reporting results to suppliers and communities; and the cost of follow-up activities. It is vital that all these elements are accurately budgeted for and cost-effectiveness achieved.
Pre-surveillance activities
Prior to the start of a surveillance programme, there are a number of activities which should be undertaken to ensure that the planners have access to all baseline data to design the surveillance programme. The pre-surveillance activities should provide the information concerning current status of water supply and surveillance in the country, and will include the following:
Current surveillance activities: scope; analytes; reliability; who is responsible; geographical spread.Inventory of supplies: type (borehole/spring/gallery/surface etc); treatment technologies; age; population served; existing quality data; source approval;
Staff assessment: numbers available; skills available; recruitment requirements; training requirements;
Surveillance infrastructure: available laboratories; laboratory equipment; on-site equipment; consumables; transport; geographical spread; computer availability; database availability.
Once this information is available the programme can be designed and will include recommendations for improving on all the above and to test appropriate methods. It is usual to run a pilot project to evaluate the approach to be adopted and to identify any parts of the programme which require improvement.
Pilot project
There are essentially two approaches to the establishment of a pilot phase that can be adopted:
1. the use of a pilot project concentrated within one geographical area;2. establishing surveillance on small scale national basis, with a small number of supplies included from each region.
Selected supplies may be restricted to those with large populations (for instance over 10,000 people or provincial capitals) or may include supplies that serve all types of population centre.
The first of these approaches allows a more intensive allocation of resources and it may be easier to measure the effectiveness of the approach adopted. However, there is a risk that the area selected may not be representative or that successful approaches may not be replicable in other parts of the country. This may be due to different types of source or treatment used, different staffing structure or resource base. It may be difficult to develop and sustain the level of support available for a small regional, pilot-scale project on a national scale in the short term. Different regional water suppliers may have different priorities based on the principal threats to water quality in each region, the surveillance infrastructure available, the expertise available and the number of people served.
A national pilot project may be more expensive due to increased travel costs and may be difficult to manage. However, there are many advantages in this approach. It is much easier to establish a large-scale national surveillance programme if in the pilot phase a national approach was adopted. In this way, difference in priorities between regions will have been identified at an early stage and can be incorporated within the national plans. It will highlight any logistical, staffing or infrastructural problems that exist in a region and these can be planned against in the full programme. This approach is also likely to permit all types of water source and supply found in the country to be represented in the pilot phase, something that may be difficult to achieve in a single region.
Once the pilot project is complete and modifications made as required, the surveillance programme proper can start. The implementation of surveillance is likely to be staged over a number of years and short, medium and long term plans will have to be drafted.
Short-term plans
The short-term aim for a water surveillance programme should be to establish it as a perceived key priority of water supply and water resource management and to create an environment which actively promotes surveillance.
The short-term objectives of national surveillance programmes should be to achieve routine analysis of critical parameters covering a representative sample of all water supplies. There are no hard and fast rules determining this, but a figure of around 30 per cent of all water supplies has been adopted in some circumstances. If only a proportion of supplies is to be included initially, the supplies should be spread geographically, encompass examples of all (or at least the principal) source types and treatment technologies and should be concentrated on communities with larger populations. Given that protected groundwater sources tends to have less bacteriological contamination, it is common to include a greater proportion of surface supplies in the early stages of surveillance. Supplies where there are known problems with water quality should be included at this stage to try to establish the causes, rectify these and prevent their recurrence.
Where chlorinated water supplies are surveyed, from whatever source, turbidity and chlorine residual within the network should be tested regularly. As the equipment and consumables required are very cheap and testing is field based, it is feasible to test frequently and this may help reduce the number of microbiological samples required.
The number of microbiological samples taken and their frequency will vary depending on resources and population size, but as far as possible samples should be taken at least quarterly by the supplier and at least annually by the surveillance agency. The number of samples taken is largely dependent on population supplied, time available, analytical resources and type of distribution network. However, the more samples that are taken, the more representative the results. Below is a very crude guide for the minimum number of samples that should be taken:
|
Populations below 5,000 |
5 samples - 1 at treatment works outlet, 1 at storage tank, 3 in the distribution network; |
|
5,000 - 10,000 |
7 samples - 1 at works outlet, 1 at storage tank and 5 in the network; |
|
Over 10,000 |
7 samples + 1 extra sample per 5,000 population - 1 at works outlet, 1 at storage tank, rest in network. |
If water supplies are from a point source, for instance a borehole or well, not connected to a pipe network, analysis need not be as regular. However, there should be a minimum of two analyses per year - one wet season and one dry season - to take into account water level fluctuations and to assess whether quality varies seasonally.
Sanitary inspections should be carried out regularly by the supplier or the community on all water supplies and not merely those where analysis is being carried out. Sanitary inspections may be undertaken by staff such as systems operators or by trained community members.
Where there is a supply agency responsible for the provision of drinking-water, the results of the sanitary inspection and any recommendations for action should be noted and shared with the supply agency. An annual summary of inspection results should be passed to the surveillance agency which highlights any actions which have been recommended and the outcome of these.
Where the water supply is community managed, the results of the sanitary inspections should be used by them to plan improvements to their supply and an annual summary of the results should be passed to the surveillance agency. An annual independent sanitary inspection by the surveillance agency should also be carried out.
Training programmes should be initiated to ensure that staff are able to carry out surveillance activities and can pass on skills in sanitary inspection to communities. Staff from both the suppliers and the surveillance agency are likely to require training, as are any community members involved in surveillance.
Medium-term plans
The medium-term aim of surveillance should be to review and consolidate the programme and expand it to cover a greater proportion of water supplies and to ensure that adequate standards are established.
One of the medium-term objectives of water surveillance should be to increase the coverage of the surveillance programme and to make modifications to the programme as appropriate. The proportion of supplies that have regular analysis of critical parameters should be increased, for example to 80 per cent. The additional water supplies included in the surveillance programme should be distributed to reflect population distribution and the number of groundwater supplies covered increased.
Chlorine residual and turbidity testing in the distribution network should continue to include all chlorinated water supplies and the frequency of testing increased. The number of samples taken from the distribution network for microbiological analysis should be increased and the supplier should aim to carry out microbiological analysis of samples at least quarterly and preferably monthly on large supplies. An independent analysis by the surveillance agency should be carried out at least annually or even more frequently on large supplies. The analytical range may also be extended to include other parameters such as total coliforms or other faecal indicator bacteria.
Lines of communication should be established between supplier, consumer and surveillance agency and the population should be kept aware of water quality problems that arise and precautionary actions that they should adopt.
Quality standards may be revised or if in the initial phase employed the use of guideline figures for water quality, the second phase may well include adoption of legally binding water quality standards. Standards or guidelines for other substances of health importance, for instance nitrate, should be drafted and analysed for as frequently as feasible.
Sanitary inspections should continue to be carried out monthly by the supplier at all supplies and independent inspections carried out at least annually. Larger supplies and a significant number of other supplies should be inspected quarterly by the surveillance agency.
In addition, codes of practice and construction standards for plumbers and builders should also be established and supported within the legal framework. A system for licensing approved craftsmen should be established with them regularly assessed and if consistently blow acceptable standards, a mechanism established to revoke their licenses.
An on-going training programme for staff involved in surveillance should be established and cover analytical techniques, sanitary inspection techniques and community education. This should include ensuring that appropriate courses are offered and made accessible for staff with extensive experience but limited formal qualifications. In-service training in appropriate topics should be provided and taught through short-courses and 'on-the-job' training.
The national laboratory network should be increased and appropriate AQC procedures established to ensure analytical quality is maintained.
Long-term plans
The long-term expansion of the surveillance programme should be to include all water supplies in the country in the surveillance programme and to ensure that both the supplier and the surveillance agency undertake regular sampling and sanitary inspection. The long-term surveillance plan should include the assessment and revision if necessary of drinking water quality standards and these should be expanded to cover all substances of health and environmental importance.
Samples should be taken monthly for microbiological analysis and in larger supplies this should be expanded to weekly or daily. the surveillance agency should aim to undertake regular independent analysis. The number of samples taken from the distribution network for microbiological analysis should be increased and should be representative of the entire network.
Sanitary inspections should be carried out by the suppliers on a monthly basis on larger supplies and at least quarterly on smaller supplies with independent inspections carried out quarterly or bi-annually. In chlorinated supplies, the supplier should sample for turbidity and chlorine residual at least weekly and in large supplies daily.
As in each phase of the surveillance programme, there must be clear lines of communication between supplier, consumer and surveillance agency. Legislation should be drafted which gives a framework of the steps to be taken by the supplier to inform the consumers and the surveillance agency when water quality is sub-standard. This should include time limits within which contamination must be reported and advice given about precautionary actions that should be taken by the consumer (for instance boiling). There should also be time limits imposed within which the surveillance agency should be informed of any failure to meet standards and proposed action.
Full analytical quality control and assurance procedures should be established and all laboratories where analyses are undertaken should be part of analytical quality control and analytical quality assurance programmes. A national reference centre should be established, possibly supported by a network of regional centres. There should also be clear guidelines for ensuring the analytical quality and reliability of results obtained from on-site equipment.
A human resource development strategy should be drafted which identifies sector training needs and how best training should be provided. This should include in-service training and establishment if appropriate of further and higher education courses which will produce appropriately qualified staff.
Conclusion
Monitoring and assessment of microbiological water quality is a key priority in the water sector which involves water suppliers, surveillance agencies and communities. It is a health-based activity and should include elements of hazard identification and risk assessment, through the use of systematic sanitary inspection, as a means of improving water supply quality.
Analysis of indicator bacteria should be supported by turbidity and chlorine residual testing and these elements, combined with sanitary inspection, should be used to define the sanitary status of the water supply.
Monitoring is best implemented through a series of stages to ensure that any problems in implementation are identified and rectified during the early stages of programme development. Initial pilot projects should test the methodology to be used and this should then be progressively implemented on a nation-wide basis.
References
Anon. Guidelines for Drinking Water Quality. Volume 3 (2nd Edition). WHO, Geneva 1997
Bartram, J. (1996) Optimising the Monitoring and Assessment of Rural Water Supplies. PhD Thesis, University of Surrey.
Bartram, J. and Balance, R. (1996) Water Quality Monitoring. Chapman and Hall, London
Howard, G. Developing Drinking Water Quality Monitoring in Zimbabwe, ODA Project Reports 2-7, National Water Quality Analysis Laboratory
Howard, G. (1997) Water Quality Monitoring: Key Issues and Approaches. Waterlines (in press)
Lloyd, B. and Helmer, R. (1991) Surveillance of Drinking Water Quality in Rural Areas. Longmans' London
Lloyd, B., Bartram, J., Rojas, R., Pardon, M., Wheeler, D. and Wedgwood, K. (1991) Surveillance and Improvement of Peruvian Drinking Water Supplies. ODA. Guildford.
Presentation Plan
|
Section |
Key points |
OHP |
|
Introduction |
· routine monitoring and assessment of microbiological quality is the key priority for suppliers and surveillance agencies |
1,2,3 |
| |
· microbiological contamination represents an acute risk to health and the health-based monitoring of water quality is crucial | |
| |
· in order to safeguard health, other parameters of water supply quality should also be monitored including quantity, continuity, coverage and cost as well as water quality | |
| |
· the water suppliers should monitor compliance with national standards and regulations within their area of service | |
| |
· the surveillance agency should monitor water supply to all the population and identify unserved or under-served areas and promote improvements |
|
|
|
· hazard identification and risk assessment should be included in sanitary inspection and should be systematic and quantifiable | |
| |
· source protection and minimum treatment requirements are also key complementary activities | |
|
Planning monitoring and assessment |
· monitoring and assessment only effective when well planned and implemented |
4,5,6 |
| |
· monitoring of microbiological quality of water supplies must have key health related objectives which aim to maintain or improve water supply quality | |
| |
· surveillance is the combination of sanitary inspection and water quality analysis and is essentially health-based water supply monitoring |
|
|
|
· monitoring and surveillance activities should be well planned if there are to be effective | |
| |
· it is important to develop monitoring programmes in stages to allow refinement of the programme with time | |
| |
· this is particularly true where monitoring has not previously existed | |
| |
· it is important to use pilot projects to test the approach proposed before any large scale implementation is undertaken | |
| |
· the most sustainable approach to monitoring is one where short, medium and long-term plans are prepared from the outset | |
| |
· initial priority should be given to those supplies which serve large populations | |
| |
· all monitoring should be linked to improvements in water supply through identifying of appropriate preventative and remedial actions |
|
|
Analytical ranges |
· this has led to the concept of the critical parameters by WHO |
7,8 |
| |
· these are: thermotolerant coliforms, chlorine residual, turbidity and pH | |
| |
· when developing monitoring initially concentrate on the critical parameters | |
| |
· only expand the analytical range once full coverage of supplies with critical parameters has been achieved | |
| |
· selection of new parameters should be these which either directly affect health or cause water supply rejection by consumers | |
|
Design of networks |
· the design of sampling networks should be well planned and done on the basis of a detailed knowledge of the water supply |
9,10,11 |
| |
· sample sites must be representative of the: source; treatment plant; storage tank; household connection; and point of use. |
|
|
|
· especially in early stages, it is important to take samples from points where it is known or suspected that problems exist | |
| |
· ensure samples are taken from main lines, remote branches and dead ends | |
| |
· use supply zones in large supplies | |
| |
· sample sites may be classified in a number of ways | |
| |
· fixed samples are useful to pick up long term water quality variation and thus indicate whether a source or treatment plant is sustainable |
|
|
|
· variable sites will pick up local and transient problems with water quality | |
|
Sampling frequencies |
· minimum sampling frequencies have been defined by WHO for piped and point water sources |
12,13 |
| |
· where possible, sampling frequency should be increased |
|
|
|
· it is often better to develop a few well functioning monitoring networks which actively contribute to water supply improvement to the basis for later development | |
| |
· costs may be reduced in piped water supply by focusing monitoring on chlorine residual and turbidity | |
| |
· where chlorine residual is <5TU and free chlorine residual>0.2mg/l it is very unlikely that faecal coliforms will be present and a test may not be necessary | |
| |
· if this approach is adopted, some random samples for faecal coliform analysis should still be taken | |
|
Linking monitoring to improvement |
· water quality monitoring should be linked to improvement in water supply by identifying remedial and preventative actions |
14 |
| |
· when planning interventions, it is likely to be necessary to prioritise supplies and actions on the basis of greatest risk | |
| |
· thus systems which classify water quality and sanitary risk in broad quality groups are useful to identify supplies which present the greatest risk to health | |
| |
· on larger scales (including national) water supplies can be ranked on the basis of greatest risk and these can be prioritised for action |
|
Why Monitor?
· Protection of human health
· Compliance with standards and guidelines
· Situation analysis/impact assessment
· Environmental change and trends
· Rapid detection of faults and failure
· Prioritisation of remedial actions
· Adequate quality of service
Five Key Elements for a Water Supply
· Quantity: Enough water for everyone to drink, cook and bath, e.g. 30-100 litres/person/day· Quality: The water will not cause disease in those drinking or using it
· Cost: The cost of sufficient water for basic needs is within everyone's reach
· Coverage: Water is available to everyone in the community
· Continuity: Water is available all day, every day
All five elements are vital if health is to be improved and maintained
Ensuring Microbiological Quality
· Source protection
· Minimum treatment requirements
· Sanitary inspection
· Water quality analysis
Objectives of Water Quality Monitoring
· Evaluate risks to the population
· Improve the situation
· Determine long-term trends
· Prioritise interventions

Developing Water Quality
Monitoring
Water Quality Surveillance
'...the keeping of a careful watch at all times, from the public health point of view, over the safety and acceptability of drinking-water supplies'
(WHO, 1985)
· Source
· Treatment
· Distribution
Coliform Analysis + Sanitary Inspection = Surveillance
Selection of Parameters
· First Stage
» Critical parameters (WHO)
» Organoleptic parameters (taste, odours, colour)
» Known problem of public health concern
· Expansion of Analytical Range
» Should be the objective only once critical parameters are being used and improvements are being made
· Selection of New Parameters
» Those parameters which affect health
» Those parameters which lead to rejection of supply by consumers
The expansion of the range of parameters must be progressive and allow priorities to be identified
Critical Parameters
|
Parameter |
Acceptable range |
|
Feacal coliforms |
0/100 ml |
|
Turbidity |
< 5 NTU |
|
Disinfectant residual |
0.2-0.5 mg/l |
|
pH |
6.5-8.5 |
Samples must be analysed within 6 hours of taking the sample form a water supply. In areas where transport or roads are poor and this is not possible, portable water testing kits can be used
Design of Surveillance Networks
· Site selection representative of:
» Water source
» Treatment plant
» Storage tank
» Household connection
» Point of use
· Look at where problems are likely to occur:
» Main lines
» Remote branches
» Dead ends
· Use 'zoning' for large systems with several sources.

Sampling Network Design (Small
supply)
Sample sites in a small water supply with ring main
Sampling Network Design (Large
supply)
Sample sites on a large supply with an open network
Classification of Sample Sites
· Fixed - Agreed in consultation with supply agency
» To help surveillance agency and water supply agency to compare results
» Allows legal action to be used to ensure improvement
· Fixed - No consultation with water supply agency
» Used with other fixed sites to determine changes in water quality with time
· Variable - Samples taken at random by surveillance agency
» Good for identification of local problems e.g. complaints, leaks
» Could include 'points of use' sampling
Minimum Sampling Frequency for Water Supply Systems
|
Population served |
Minimum frequency |
|
< 5000 |
1 visit each month |
|
5000 -100 000 |
1 visit for every 5 000 population each month |
|
> 100 000 |
20 visits each month plus 1 visit for every |
| |
10 000 population every month |
Using monitoring to improve water
supplies
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Monitoring and Assessment of Chemical Quality
Session Objectives
· To highlight the relative priority for microbiological and chemical water quality monitoring and emphasis the need for a rational, health-based approach to monitoring of water quality.· To outline the key characteristics of monitoring programmes which may be implemented for chemical water quality.
· To describe the analytical ranges commonly employed in chemical water quality monitoring, highlight key constraints in chemical analysis and stress the need for quality control.
· To emphasis the value of risk assessment as a key supporting activity of chemical analysis and in planning monitoring programmes.
Introduction
Chemical testing is generally not undertaken as frequently as microbiological analysis because, in general, the health risks posed by chemicals are chronic rather than acute and because changes in water chemistry tend to be longer-term unless a specific pollution event has occurred. It should be stressed that monitoring the microbiological quality of water is much more important than monitoring of chemical quality and chemical testing should generally be a lower priority.
However, where resources permit, routine testing of the chemical quality of water should be undertaken. Priority should be given to those substances which are known to be of importance to health and which are known to be present in significant concentrations in drinking-water. For instance, the monitoring of nitrate is recommended in many water supplies and in particular those which are located in rural areas, or where recharge occurs in an agricultural area. In these circumstances, regular monitoring is recommended to ensure that early warning of increases is noted or when nitrate releases are highly seasonal in nature.
An assessment of the chemical quality of water should be undertaken during source selection and this should relate to known activities within the catchment of the source and possible natural pollutants. This should be as comprehensive as possible and cover a wide range of pollutants.
In areas where toxic chemicals are released into the aquatic environment, routine monitoring should be undertaken and closely linked with an emergencies warning procedure which should function to alert water suppliers, surveillance agencies and health bodies of any accidental releases of substances into water sources.
Types of monitoring programme
As with any form of monitoring, it is important that clear objectives are set before the start of data collection activities and that sample sites and frequency of analysis are determined to meet the objectives and not vice versa. In the past, some water quality assessments have worked from the other way round and monitoring programmes have been designed to fit existing infrastructure. The problem with this approach is that it very often results in a failure to address the most pressing problems and also a failure to provide a full picture of the problem being monitored.
In general, monitoring of the chemical quality of water may be undertaken in two ways.
1. Routine monitoring of known problem substances: this type of programme is designed to keep a continuous watch on substances which are known to have a health impact or compromise treatment efficiency and which are known or suspected to be in the water supply to be monitored. It is important that substances whose concentration is likely to change are monitored more regularly than those where concentrations are essentially stable. This is largely determined by the source of the contamination. Contaminants from essentially natural sources, such as fluoride, are unlikely to vary significantly over time and therefore do not require frequent analysis. Although there may be exceptions to this such as the raised arsenic levels in some groundwaters in West Bengal, India. Contaminants deriving from anthropogenic sources of pollution may require more frequent analysis, for instance heavy metals in water sources downstream of tannery waste discharges. Equally, where treatment is employed to remove or control specific substances (e.g. nitrate or phosphorous), these should be routinely monitored at the plant to ensure that treatment is effective.2. Periodic quality assessment: this type of monitoring is either routine or non-routine assessment of water quality done on a relatively infrequent basis (annual or greater). Such assessments will certainly be done during the source selection procedure and may involve periodic evaluations of trends in water quality over time. Such assessments are likely to include a wider analytical range and be used to provide regular comprehensive assessments of water quality to assist in long-term water source and supply management and for long-term trend analysis.
Both approaches will concentrate on water quality in the source and as it leaves the treatment works or borehole, with a limited number of samples taken from within the distribution system, unless the materials used in the distribution system are suspected of providing a significant proportion of a harmful substance. In these circumstances it is usually more effective to monitor and control the quality of materials and chemicals used in water treatment during their production and prior to their use. However, where materials or chemicals have been used without quality control during manufacture, some monitoring of specific chemicals may be required by the public health agency. For instance, where lead pipes or lead-based solders are used, regular monitoring of lead may be recommended.
Selection of variables for monitoring and assessment
As mentioned above, during source selection, a comprehensive assessment should be made of water quality to ensure that any likely risks to health are identified and appropriate action taken with regard to source protection, treatment requirements and blending of water. Thus analysis of the major ions and nutrients should be done on all water supplies as well as any other substances deemed likely to be present on the basis of land-use within the catchment of the source. However, whilst it is preferable to have a complete and comprehensive description of water quality before a water supply is commissioned, there are a number of constraints in trying to achieve this.
Many analyses are expensive to carry out, both in terms of the equipment required to perform the analysis and in terms of the consumable required. This means that if analysis is required for a particular analyte which uses sophisticated equipment, this may only be done occasionally when the laboratory has enough samples to make it economic to start up the equipment and run the analysis. It is never economic to start equipment such HPLC or a flame photometer to carry out a single analysis. Therefore appropriate storage facilities are required for the sample and appropriate preservatives must be available to prevent sample deterioration. This will further increase the costs of analysis.
Thus for some parameters, there may be a considerable time to wait before the results of analysis are known. However, the delay in opening the water supply, particularly in drought-prone areas, may be unacceptable. Therefore during source selection, parameters should be divided into essential and desirable. This should be done based on the risk to health, potential to cause consumer rejection, likelihood of causing operational problems, cost and ease of analysis, likelihood of presence in drinking-water.
The net result is likely to be a range of parameters which are analysed rapidly and perhaps on-site and before the source is commissioned (for instance, nitrate, fluoride, iron etc.) and those which will be done, but possibly after the source has been commissioned.
There are a number of parameters which, when used in conjunction with a pollution source assessment, provide a good overall indication of chemical water quality and others whose impact on human health or the environment are great and should be included in initial testing. The presence at high levels of these parameters in the source water may indicate that other analyses are required. These include: nitrate, pH, Eh, fluoride, dissolved oxygen and chloride.
The presence of elevated levels of nitrate in water indicates pollution of the source and it is important that the type and source of the pollution is identified. Nitrate pollution may occur from agricultural source, sewage disposal and urban runoff. Agricultural sources may indicate that there will also be a problem with other agricultural pollutants such as pesticides. It is important that a survey is carried out to identify whether there is use of pesticides in the area and to find out application rates and time of application. Pesticide analysis is difficult and expensive, indeed there are a number of pesticides for which no analytical methods exists for detection in water, therefore routine analysis of pesticides will not be carried out at the start of a programme and is rarely fully developed. Nitrate contamination which can be linked to a sewage outfall may also indicate unacceptably high levels of microbiological contamination which should be addressed as a matter of priority.
For routine analysis, both the monitoring agency and the supplier should aim to concentrate on those chemical parameters which are of greatest health significance or provide a general description of water quality and for which analysis is inexpensive, quick and may be done on-site. There are variables such as pH and Eh (redox potential) which should, by preference, be done on-site as the sample may deteriorate during transport.
Risk assessment
As with microbiological monitoring, it is important that monitoring of chemical water quality is linked to a process of hazard identification and risk assessment. Thus when designing a monitoring programme, an inventory of likely sources of pollution and the likely vulnerability of a water source or distribution system to contamination should be made. This means that information will be required on the following:
· geographical features, including topography, relief, lithology, climate, land-use, hydrology;· other water uses from the source; and
· pollution sources, treatment of wastes and discharge consents in operation.
Risk assessment should be a dynamic process which is conducted or updated routinely by suppliers and surveillance bodies to ensure that no new risks are developing for which remedial or preventative action is required. Thus, for each new activity established within the catchment of the water source used for drinking purposes, a detailed description of likely pollutants that may be discharged, wastewater treatment arrangements, recycling and discharge consents must be obtained. These should be used to allow water suppliers and surveillance bodies to object to developments which will compromise public health through likely discharges and to establish monitoring programmes which are focused on health-based risk assessment.
Chemical testing of drinking-water supplies is often linked to source quality monitoring and thus it is very important that hydrological data are collected at the same time as quality data as this has a profound influence on water quality. Flows in rivers will determine the concentration of pollutants in the aquatic environment. For instance, in the UK at low flows, up to 95 per cent of the flow of many rivers which pass through urban areas is municipal effluent, whilst at high flows this percentage will be greatly decreased and effluent may only account for 30% of the flow.
The status of rivers with regard to groundwater is also important as this will influence water quality. Hydrogeological data are also important as water level, flow patterns and water movement rates will all affect water quality. For example, changes in water level may significantly alter water quality as pollutants removed from infiltrating water in the unsaturated zone by sorption may be eluted (de-sorbed) if the groundwater level later rises.
Quality control
It is important that data generated in chemical testing programmes in different regions are comparable and that time series of data are also comparable. Therefore: standard operating procedures are required for sampling, field testing and data reporting; AQC schemes should be carried out for all laboratories carrying out analysis; field equipment should be regularly checked and calibrated; staff should be adequately trained and supervised.
Provided the same analytical techniques are used over the time period to be studied and the above are implemented, data time series should be comparable. However, as analytical techniques are continually improving and changing, it is common to find that techniques for analysing particular variables change and that the results produced are not directly comparable to previous methods. When this happens, it is important that both the new and old technique are used to analyse samples for a hand-over period to allow a conversion graph to be prepared to allow comparison of the results of both methods.
Where there are a number of laboratories involved in water quality analysis, there should, preferably be some form of inter-laboratory comparison. This may take the form of a reference laboratory provided spiked samples to laboratories in which the concentrations of chemical constituents is not known by the participating laboratories. Alternatively, laboratories can rotate quality assurance sample preparation. The purpose of such procedures is to improve the overall reliability of the data produced in water quality analysis.
Conclusion
Chemical monitoring is a lower priority than microbiological monitoring. As monitoring of chemical water quality is developed, a clear priority should be given to substances of known health impact and which are known or suspected to be in the water supply. Monitoring may be carried out routinely for some chemicals whose presence in water is likely to change over time, for which treatment is applied, or which have highly seasonal profiles. For most chemicals, and for all contaminants which have a natural source in the environment, monitoring may be done through periodic assessment of water quality.
Monitoring of chemical water quality should incorporate hazard identification and risk assessment as a key tool for managing risks. Thus, water suppliers and surveillance bodies should be aware of all potentially polluting activities within the catchment of a water source and use this information to help design monitoring programmes. Where activities involving the use or production of toxic chemicals, adequate emergency warning procedures must be established which will ensure that water suppliers and surveillance bodies are kept informed of any accidental spill into water sources.
References
Chapman, D. (ed) (1996) Water Quality Assessments. 2nd edition. Chapman and Hall.
Anon. (1993) WHO Guidelines for Drinking-water Quality, Volume 1. WHO, Geneva.
Howard, G and Simonds, A, (1995) Where there is no training - pollution risk assessment for field staff. Waterlines, Vol 14, No. 1. July 1995.
Presentation Plan
|
Section |
Key points |
OHP | |
|
Introduction |
· chemicals evaluated during the preparation of the 2nd edition of the Guidelines |
1,2,3 | |
| |
· many chemicals, such as nitrate, lead and arsenic, can be toxic to humans and may come from natural and anthropogenic sources | |
|
| |
· chemical testing not undertaken as often as microbiological testing because most health risks are chronic not acute | | |
| |
· changes in water chemistry also tend to be long-term unless specific pollution event occurs | | |
| |
· where possible do routine monitoring of chemicals of health concern and known to be in drinking-water - e.g. nitrate | | |
| |
· comprehensive assessment of chemical water quality should be done during source selection | | |
| |
· early warning procedures essential and should link resource managers, water suppliers, surveillance agency and health bodies | |
|
|
Types of monitoring programme |
· need to have clear objectives before data collection starts and monitoring network should be designed to match objectives not vice versa |
4,5 | |
| |
· where objectives are set to match monitoring programmes may fail to meet most pressing needs | | |
| |
· two key approaches to chemical monitoring | | |
| | |
1 routine monitoring of known problem substances |
|
| | |
- designed for continuous surveillance of substances of health concern and which are in water supply | |
| | |
- only routinely monitor substances where concentration likely to change because of a pollution event or treatment failure | |
| |
|
2 periodic quality assessment | |
| |
|
- either routine or non-routine assessment of water quality on relatively infrequent basis |
|
|
| |
- assessment certainly done during source selection and subsequent occasional evaluations |
|
|
| |
- such assessments likely to have a broader analytical range than routine monitoring | |
| |
· both types of monitoring tend to focus on sources and where water leaves pumping station or treatment plant unless distribution system suspected of leaching substances into the water |
| |
| |
· where substances in water are derived from chemicals and materials used to treat and distribute water, it is often better to monitor and control manufacture than in drinking-water | | |
|
Variable selection |
· preferable to have a complete description of quality of a water supply prior to commissioning, but may be problems in achieving this |
6 | |
| |
· many analytes expensive to analyse for and only economic for analysis of a limited number of samples, therefore may delay analysis |
| |
|
|
· this has implications for source commission as unacceptable in many circumstances to wait until results available for commissioning |
| |
|
|
· therefore need to identify a restricted range of analytes of health concern which can be used to indicate broader problems and which are relatively easy to analyse,e.g. nitrate and pH | | |
| |
· nitrate is of particular concern and in many circumstances is routinely monitored and source identified as this may indicate other pollution |
| |
|
|
· for routine analysis concentrate on chemicals of known health concern and can be easily monitored | | |
| |
· some parameters should be done on-site to prevent sample deterioration | | |
|
Risk assessment |
· monitoring chemical quality should also be linked to risk assessment and hazard identification |
7 | |
| |
· when assessing vulnerability make sure collect information on geographical/geological features that may increase vulnerability | |
|
| |
· during risk assessment identify all likely sources of pollution | | |
| |
· risk assessment is dynamic and should be routinely undertaken |
| |
|
|
· both supplier and surveillance agency should be aware of new activities within the catchment to predict likely impacts on water supply | |
|
| |
· need to collect hydrological/hydrogeological data as well as quality data | | |
|
Quality control |
· need to be able to compare data from different regions and time series of data | | |
| |
· therefore quality control is essential and standard operating procedures are required for sampling, analysis and reporting | | |
| |
· all equipment, including field kits, require calibration and staff trained | | |
| |
· where techniques change over time, ensure that new techniques is calibrated against old technique to ensure comparability | | |
| |
· inter-laboratory comparison is important for improving and maintaining analytical quality | | |
|
Conclusions |
· chemical monitoring is a lower priority than microbiological monitoring | | |
| |
· priority should be given to those parameters of known health concern | | |
| |
· routine monitoring should be done for parameters whose concentration is likely to vary, for which treatment is carried out or which have seasonal profiles | | |
| |
· hazard identification and risk assessment should also be carried out and an early warning system implemented | | |
Assessment of Health Risks of Chemicals in Drinking-Water
|
|
Number of chemicals considered | |
|
Inorganics |
34 | |
|
Organics | |
|
| |
Chlorinated alkanes |
5 |
| |
Chlorinated ethenes |
5 |
| |
Aromatic hyrdocarbons |
6 |
| |
Chlorinated benzenes |
5 |
| |
Miscellaneous organics |
9 |
|
Pesticides |
35 | |
|
Disinfectants |
6 | |
|
Disinfectant by-products |
23 | |
|
TOTAL |
128 | |
Chemical Monitoring
· Far lower priority than microbiological monitoring· Comprehensive assessment of water quality recommended during source selection
· Must be linked to ongoing risk assessment
· Quality control and assurance are vital for compliance monitoring
Toxic Chemicals in Water
Nitrate:
· Causes acute health effect in infants
· May be pronounced seasonal variation
· Long-term levels increasing worldwide
· Nitrate often monitored routinely
Lead:
· Link to intellectual impairment
· Main source in water likely to be from pipes/solders
· Monitor lead in water or monitor use of lead pipes
Arsenic:
· Often natural source· Release due to water table lowering (India) -arsenates are desorbed during recharge
· Release under urban areas related to waterlogging and raised pH from humic and fluvic acids
Monitoring Chemical Contaminants
· Chemicals are often difficult or expensive to remove· Chemical pollutants from natural sources tend to vary slowly
· No universal indicator chemicals have been identified unlike indicator bacteria
· Therefore, monitoring at long intervals unless:
- a health problem is identified
- treatment is applied to remove substance
- a pollution event is recorded which may affect supply
- upgrading/expansion of system is planned
Monitoring Strategies for PhysioChemical Monitoring
These vary according to parameter:
· Critical parameters (turbidity, pH, chlorine residual) routine analysis· Known/suspected problem with particular substance (nitrate, THM, etc.) - routine analysis
Other parameters are analysed on an occasional basis:
· If their presence is suspected at harmful levels (e.g. fluoride)· During source selection and infrequently afterwards
· Once problem and scale is identified there is no value in regular monitoring as levels unlikely to change quickly.
Physio-Chemical Monitoring
Parameters:
· Temperature
· pH
· Conductivity
· Redoxpotential (Eh)
· Turbidity
· Total suspended solids
· Total dissolved solids
Chemical compounds such as:
· Chlorine residual
· Nitrate
· Fluoride
· Arsenic
· Aluminum
· Lead
· THMs
· Some pesticides, etc..
Risk Assessment
· Risk assessment should be ongoing· Initial assessment during source selection should identify potential sources of pollution
· Pollution risks assessment should be carried out whenever a new activity starts
· Regular assessment will support analytical work
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Guidelines for Drinking-Water Quality Volume 3
Session Objectives
· To describe the scope, purpose and content of Volume 3 of the Guidelines for Drinking-water Quality and the process of it's development.· To describe the basic concepts incorporated within Volume 3 of the Guidelines and show how these should be addressed within the context of monitoring development.
· To describe the implementation of surveillance programmes in small communities and to emphasise the use the use of sanitary surveys, source protection and minimum treatment requirements in these areas.
History and Development
The first edition of WHO Guidelines for Drinking-water Quality was published by WHO in 1984-1985 and was intended to supersede earlier European and international standards. Volume 1 contained guideline values for various constituents of drinking-water and Volume 2 the criteria monographs prepared for each substance or contaminant on which the guideline values were based. Volumes 1 and 2 of the Guidelines are therefore intended to be supportive of risk assessment. In translating the information they contain into risk management, largely through standard-setting, Member States are encouraged to take social, economic and cultural factors into consideration.
Volume 3 was concerned with the monitoring and management of drinking-water in small communities, particularly those in rural areas - a problem of world-wide concern. In contrast to the first two volumes it therefore includes relatively extensive coverage of technical, managerial and organizational aspects.
A number of important principles were established in the first edition of Volume 3 of the Guidelines, published in 1985. These included:
· the distinct and complementary roles of the water supplier and the surveillance agency;· the unique nature of the problems associated with the monitoring of small community supplies;
· the central role of microbiological monitoring of supplies of this type, including the concept of critical parameter testing; and
· the importance of ensuring that surveillance leads to engineering improvements and other remedial measures.
· It also noted the importance of remedial measures and of community participation.
During the International Drinking-water Supply and Sanitation Decade 1981 - 1990 considerable experience was gained in the surveillance and improvement of small community supplies. The first edition of Volume 3 of the Guidelines for Drinking-water Quality provided a basis for a number of pilot projects and country programs in central and south America, Africa and various parts of Asia and the Pacific, several with the support of the Overseas Development Administration of the United Kingdom (ODA) and the United Nations Environment Program (UNEP). Regional and national training courses were conducted which were also supported by the Danish International Development Agency (DANIDA) and which allowed for the review and evaluation of the approaches and materials proposed in the Guidelines. In particular the experience gained through three demonstration projects supported in part by WHO in Indonesia, Peru and Zambia was reviewed and published in 1991.
Experience gained during the Decade highlighted the importance of additional concepts which were integrated into the second edition of Guidelines Volume 3. These included:
· the need to consider water quality not in isolation but as one of a number of water supply service parameters which influence health;· an understanding of the linkages between monitoring and improvement which then provided the structure of the document;
· the fundamental importance of sanitary inspection and of its systematization;
· practical means to compare and present information on supply service quality to assist in decision-making; and
· the importance of addressing small community supplies of all types, including those to small peri-urban settlements.
· And the second edition therefore also included increased attention to human resource development and communication issues.
The preparation of the second edition of the Guidelines Volume 3 was made possible through a grant provided by ODA to the Robens Institute, University of Surrey, UK and through the support of DANIDA to the second review meeting. The process began at a review meeting held in Harare, Zimbabwe 24 - 28 June 1991, when proposed changes were reviewed and a detailed outline agreed. A draft of the revised Volume 3 was reviewed at the Final Task Group Meeting on the Revision of the WHO Guidelines for Drinking-water Quality held in Geneva 21 - 25 September 1992. That meeting endorsed the general content of the draft, made specific recommendations for finalisation and recommended that a revised draft be reviewed at a technical meeting in Tirana in 1993 before publication. The final version of Volume 3 reflected the experience of the three demonstration projects in Indonesia, Peru and Zambia and many other projects concerned with improving the quality of water services undertaken during the Decade.
Scope and Applicability of Volume 3
Volume 3 of the Guidelines specifically addresses the specific problems associated with the surveillance of 'community supplies'. The precise definition of a 'community water supply' will vary. Whilst a definition based upon population size or type of supply may be appropriate under many conditions, it is often administration and management that set aside community supplies. The involvement of ordinary, often untrained and sometimes unpaid community members in the administration and operation of water supply systems is often characteristic of small communities and this provides already distinction between community water supplies and those of larger towns and cities. However water supplies in peri-urban areas around larger towns and cities may be organizationally similar to those of rural communities and may also be classified as 'community water supplies'.
In addition to the voluntary and local nature of the operation and management of many community supplies, they present additional challenges to the surveillance function. These challenges include the fact that the quality control function which would normally be undertaken by the supply agency may be entirely absent - a local volunteer is unlikely to be able to undertake analytical quality control - and the role of the surveillance agency may have to be modified accordingly.
Similarly, especially rural community supplies are often disperse and sometimes distant from the bases of operation of the surveillance agency. Organizing programs of regular visits to such communities presents a particular challenge and may be costly.
Finally, evidence clearly indicates that microbiological contamination is the principal health concern for community water supplies world-wide. Since microbiological contamination may vary widely and rapidly, approaches based upon sampling and analysis may be entirely inadequate in such supplies and great reliance must be placed upon preventive measures and sanitary inspection in order to ensure microbiological safety.
While conditions vary between countries and regions, as a result of differences in economic, geographical, cultural and social conditions, the strategies and procedures described in Volume 3 should be widely applicable.
Content and Structure
Volume 3 describes the methods employed in the surveillance of drinking-water supply and quality in light of the special problems of small-community supplies and outlines the strategies necessary to ensure that surveillance is effective. It is also concerned with the linkages between surveillance and remedial action and with the form that remedial action should take.
The structure of Volume 3 reflects the principal stages in the development of surveillance and in shown in Figure 1 below.

Figure 1: Structure of Volume 3 of
the GDWQ
Chapter 2 covers planning and subsequent chapters deal with the procedures used in the collection of information - sanitary inspection and community surveys (Chapter 3), and the analysis of water quality (Chapter 4). Chapter 5 considers the analysis and interpretation of the information gathered and its use in improving water supply services. The final three chapters cover strategies for improvement - technical interventions (Chapter 6), hygiene education (Chapter 7) and legislation and regulation (Chapter 8).
Basic Concepts
The distinct and complementary roles of the water supplier and the surveillance agency
Organizational arrangements for the improvement of water supply services should take into account the vital and complementary roles of the agency responsible for surveillance and the water supplier.
In most countries the agency responsible for surveillance of drinking-water supply services is the Ministry of Health and its regional or departmental offices. In some countries there is an environmental protection agency; in others environmental health departments of local government may have some responsibility. Its responsibilities should encompass: the monitoring of compliance with supply service standards including quality, coverage, quantity, continuity and cost by water suppliers; approving sources of drinking-water, and; surveying the provision of drinking-water to the population as a whole.
The surveillance agency should be given the necessary powers to administer and enforce laws, regulations and codes concerned with water quality. Surveillance is indispensable for the development of rational strategies for the improvement of the quality of water-supply services.
Water suppliers should be responsible at all times for the quality and safety of the water that they produce, and they achieve this through a combination of good operating practice and preventive maintenance, supported by quality control. Water quality control is the responsibility of the supplier and involves the establishment of safeguards in the production and distribution of drinking-water as well as routine testing of water quality to ensure compliance with national standards.
Quality control is distinguished from surveillance on the basis of institutional responsibilities and the frequency of monitoring activities conducted. The surveillance agency is responsible for an independent (external) and periodic audit of all aspects of safety, whereas the water supplier is responsible at all times for regular quality control, and for the monitoring and ensuring safe operations.
These two functions - surveillance and quality control are best performed by separate and independent entities because of the conflict of interests that arises when they are combined.
The central role of microbiological monitoring
As noted above, evidence clearly indicates that microbiological contamination is the principal health concern in community water supplies world-wide. Furthermore, since microbiological contamination may vary widely and rapidly, approaches based upon sampling and analysis may be entirely inadequate in such supplies and great reliance must be placed upon preventive measures and sanitary inspection in order to ensure microbiological safety.
There are three principal components to the strategy which should be adopted and promoted. Firstly, systems should be intrinsically well-designed and capable of supplying safe water continuously. For groundwater sources this is generally achieved through source protection measures; whilst for surface water sources the selection of treatment processes and system capacity should take into account the quality and quality variations in the source water.
Secondly, regular inspections should be made to ensure that the system continues to operate safely. These sanitary inspections should take account of the whole of the supply system - from source to point of supply; and should systematically assess the condition of the system. Considerable information is included in Volume 3 including examples of sanitary inspections forms for adaptation to local circumstances. Sanitary inspections may be performed by both the surveillance agency and by the community itself. Community inspections help to ensure a higher frequency of surveillance activity than the surveillance agency itself might be able to perform. When sanitary inspections are carried out, they must use standardized methodologies to allow the consolidation of data at regional and national levels in order to prioritize interventions and investment on the basis of greatest need.
Finally, not all sources of contamination are detected by sanitary inspection, however carefully performed, and it is therefore essential to undertake occasional sampling and analysis for the critical parameters of drinking-water quality.
The importance of ensuring that surveillance leads to improvement
For water supply surveillance to lead to improved drinking-water supply services it is vital that the mechanisms for promoting improvement are recognized and used. Information alone does not lead to improvement. It is the effective management and use of the information generated by surveillance that makes possible the rational improvement of water supplies - where 'rational' means that available resources are used for maximum public health benefit.
The ways in which surveillance may lead to improvements in water supply provision are dealt with in some detail in chapters 5 to 8 and are summarized in Table 1 below which is taken from Volume 3.
Table 1: Mechanisms for the improvement of water-supply services based on the results of water-supply surveillance
|
· Establishing national priorities When the commonest problems and shortcomings in water-supply systems have been identified, national strategies can be formulated for improvements and remedial measures; these might include changes in training (of managers, administrators, engineers, or field staff), rolling programmes for rehabilitation or improvement, or changes in funding strategies to target specific needs. · Establishing regional priorities Regional offices of water-supply agencies can decide which communities to work in and which remedial activities are priorities; public health criteria should be considered when priorities are set. · Establishing hygiene education Not all of the problems revealed by surveillance are technical in nature, and not all are solved by supply and construction agencies; surveillance also looks at problems involving private supplies, water collection and transport, and household treatment and storage. The solutions to many of these problems are likely to require educational and promotional activities coordinated by the health agency. · Enforcement of standards Many countries have laws and standards related to public water supply. The information generated by surveillance can be used to assess compliance with standards by supply agencies. Corrective action can be taken where necessary, but its feasibility must be considered, and enforcement of standards should be linked to strategies for progressive improvement. · Ensuring community operation and maintenance Support should be provided by a designated authority to enable community members to be trained so that they are able to assume responsibility for the operation and maintenance of their water supplies. |
Parameters of water supply service quality
While the safe quality of water supplied to communities is an important consideration in the protection of human health and well-being, it is not the only factor that affects the health of consumers. Access to water is of paramount concern and other factors such as the population served, the reliability of the supply and the cost to the consumer must therefore be taken into account. At the United Nations Conference at Mar del Plata in 1977 which launched the International Drinking-water Supply and Sanitation Decade, this philosophy was unambiguously and the Conference Declaration included the statement that: 'all peoples, whatever their stage of development and social and economic condition have the right to have access to drinking-water in quantities and of a quality equal to their basic needs'.
Access to water may be restricted in several ways, e.g. by prohibitive charges, daily or seasonal fluctuations, breakdown, or lack of supplies to remote areas. Seasonal, geographic and hydrological factors may conspire to deprive households, communities or regions of a continuous, reliable supply of safe drinking-water. Such problems are not confined to poorer countries: they are also experienced in industrialized countries where the management of demand has failed or population growth has outpaced the rate of development of water resources for example.
If the performance of a community water supply is to be properly evaluated a number of factors must be considered. Quantitative service indicators for this purpose may include:
|
quality |
the proportion of samples or supplies that comply with guideline values for drinking-water quality and minimum criteria for treatment and source protection |
|
coverage |
the percentage of the population that has a recognizable (usually public) water supply system |
|
quantity |
the average volume of water used by consumers for domestic purposes (expressed as liters per capita per day) |
|
continuity |
the percentage of the time during which water is available (daily weekly or seasonally) |
|
cost |
the tariff paid by domestic consumers |
Need to address the population as a whole/all community supplies
It is those persons with inadequate or no water supply who are at greatest public health risk. It is technically possible, effective from a public health viewpoint and ethically desirable to identify such populations and to target them for improvements. Thus whilst the supply agency should be responsible for the quality of the service they provide, the surveillance agency should seek to assess the water supply to the population as a whole - including identifying the extent of supply within 'supplied' communities, identifying communities with no supply and determining the means of provision employed by the 'disperse' population.
Implementation
Surveillance is an investigative activity undertaken to identify and evaluate factors associated with drinking-water which could pose a risk to health. Surveillance contributes to the protection of public health by promoting improvement of the quality, quantity, coverage, cost and continuity of water supplies. It is also both preventive - detecting risks so that action may be taken before public health problems occur - and remedial identifying the sources of outbreaks of waterborne disease so that corrective action may be taken promptly.
Surveillance requires a systematic program of surveys that combine sampling and analysis, sanitary inspection and institutional and community aspects.
Conclude presentation with a summary:
This presentation has covered:
· the history of Volume 3, its special character and purpose in addressing a specific problem of world-wide concern.· the key principles underlying the volume and concerning surveillance of community supplies.
· the structure and content of volume and how it relates to the implementation of a surveillance program.
Presentation Plan
|
Section |
Key points |
OHP |
|
History and Development |
· first edition of the GDWQ published 1984-5 in 3 volumes |
1,2,3 |
| |
· volume 1: guidelines; volume 2: criteria and supporting information; volume 3: community water supplies |
|
| |
· volumes 1&2 provide risk assessment, whilst volume 3 emphasises implementation in small community water supplies and covers other aspects |
|
|
|
· 1st edition established key principles (see OHP2) | |
| |
· in IWSSD (1980s) considerable experience in small community water supplies and pilot projects used to test and refine volume 3 | |
| |
· this led to additional concepts included in volume 3 |
|
|
|
· volume 3 reviewed at 2 meetings and finally Tirana in 1993 |
|
|
Scope and applicability of Volume 3 |
· volume 3 specifically addresses community-based water supplies |
4 |
| |
· community supplies defined on the basis of management/administration rather than population size or type of supply | |
| |
· community supplies may cover both peri-urban and rural water supplies operated and managed by non-professional community members |
|
|
|
· community water supplies present unique monitoring problems, there is often no quality control function and thus modified surveillance role |
|
|
|
· rural communities often dispersed and many in number making surveillance costly | |
| |
· need to emphasise preventive actions and non-analytical approaches to surveillance to ensure microbiological quality | |
|
Content and Structure |
· volume 3 outlines methods for surveillance in community water supplies and in particular the linkage of surveillance to improvement of water supplies |
5 |
| |
· the structure of the document reflects the stages of surveillance development for community supplies | |
|
Basic Concepts |
Distinct and complementary roles of supplier & surveillance agency |
6,7 |
| |
· institutional structure of the water sector must recognise the vital and complementary roles of suppliers and surveillance agencies | |
| |
· surveillance usually done by MoH, but sometime by MoE or local government and should encompass quality, quantity, continuity, coverage and cost | |
| |
· surveillance agency should enforce water laws and use monitoring data to improve water supplies | |
| |
· water suppliers responsible for quality control of water they supply | |
| |
· surveillance is independent audit of water supply | |
| |
· should separate institutions undertaking quality control and surveillance to prevent conflict of interest | |
| |
Central role of microbiological monitoring | |
| |
· microbiological contamination is principal health concern in community water supplies | |
| |
· microbiological contamination may vary widely and rapidly, therefore analytical approaches alone are not adequate | |
| |
· sanitary inspection and preventive measures are essential |
8,9,10,11 |
| |
· approaches to community water supply should ensure that: | |
| |
a) systems are well-designed to provide safe water continuously (source protection & minimum treatment) | |
| |
b) regular sanitary inspection carried out on all system to ensure risks rapidly identified and eliminated | |
| |
c) occasional water analysis carried out of critical parameters | |
| |
Importance of linking surveillance to improvement |
|
| |
· surveillance must link to improvement and mechanisms to achieve this must be identified | |
| |
· information alone is not sufficient, but the rational use of information for improvement of water supplies (prioritisation, identification of faults etc.) | |
| |
Parameters of water supply | |
| |
· must address all aspects of water supply | |
| |
· access must be seen as the key priority | |
| |
· also take reliability, coverage and cost into account |
|
|
|
· there can be many reasons why access to water supplies may be restricted | |
| |
· when evaluating performance of community water supplies, can use five quantitative indicators: quality, quantity, continuity, coverage & cost | |
| |
Need to address community as a whole | |
| |
· those parts of population with inadequate or no water supply at greatest risk | |
| |
· should target these groups for investment | |
| |
· supply agency responsible for ensuring adequacy of supply to the 'supplied' population | |
| |
· surveillance agency should assess whole population, identify those not supplied and determine mechanisms to rectify this | |
|
Implementation |
· surveillance is an investigative public health-based activity | |
| |
· surveillance protects health through promoting improvement in water supply | |
| |
· it is both preventive and remedial | |
| |
· surveillance is systematic and includes analysis, inspection, institutional and community aspects | |
|
Conclusions |
· have covered summary of volume 3 | |
| |
· shown the principles underlying volume 3 | |
| |
· provided structure and content of volume 3 & its implementation |
|
WHO Guidelines for Drinking-Water Quality
|
Volume 1 |
Recommendations |
|
Volume 2 |
Health Criteria and other Supporting Information (IPCS) |
|
Volume 3 |
Surveillance and Control of Community Supplies |
Principles Underlying Volume 3
· Suppliers and surveillance agency have distinct and complementary roles· Small & community water supplies have unique require a different approach to monitoring
· Critical parameter testing is of paramount importance
· Surveillance must be linked to improvements in water supply
· Many small supplies are community managed and therefore community participation is essential
Lessons learnt during the IDWSSD
· Key parameters: quantity; quality; continuity; coverage; and cost· Linkages between monitoring and improvements must be clearly understood
· Sanitary inspections are essential and should be systematic
· Water supply monitoring data must be comparable to be of use
· Community supplies, including those inperi-urban areas, must be addressed
· Human resource development and communication of monitoring information are vital
Scope and Applicability of Volume 3
· Specifically addresses community-based water supplies· Community supplies may cover both peri-urban and rural water supplies operated and managed by nonprofessional community workers
· Community water supplies present unique monitoring problems often with no quality control
· Rural communities often numerous and dispersed thus making surveillance costly
· Need to emphasise preventative actions and nonanalytical approaches to surveillance to ensure microbiological quality

Structure of Volume 3 of the
GDWQ
Distinct and complimentary roles of
suppliers and surveillance agencies

Strategy for water supply quality
protection and improvement
Critical Parameters
|
Parameter |
Recommended Level |
|
Faecalcoliforms |
0 per 100 ml |
|
Turbidity |
<5 NTU |
|
Disinfectant residual |
0.2 - 0.5 mg/l |
|
pH |
6.5 - 8.5 |
Note: Samples must be analysed within six hours of taking the sample from a water supply. In areas where transport or roads are poor and this is not possible, portable water testing kits can be used.
Use of monitoring data to improve water supply
· Establishing national priorities· Establishing regional priorities
· Establishing hygiene education
· Enforcement of standards
· Ensuring community operation and maintenance
· Human resource development and communication of monitoring information are vital
Five Key Parameters of Water Supply Service
· Quality· Coverage
· Quantity
· Continuity
· Cost

Human Resources Development for
Water Supply Surveillance in Peru
Source: Lloyd et al., 1991
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Source Protection
Session Objectives
· To describe the need for the protection of water sources and resources.· To define the terms 'source protection' and 'resource protection'.
· To discuss the influences on quality of water in the environment and the importance of human activities on water quality deterioration.
· To describe some of the preventative measures that are applicable to groundwaters.
· To describe some of the preventative measures that are applicable to surface waters.
Introduction
The prevention of water contamination is always preferable to attempting to remove contamination once it has entered the aquatic environment. Whilst it is likely that some contamination events will always occur, a large proportion of drinking-water quality problems can be prevented through: adequate source protection and good water resource management; good design, operation and management of water supplies; and regular and thorough surveillance activities.
The initial selection of a source for drinking-water should ensure that the best source is selected. This can be done by carrying out a thorough analysis of source water quality and making a comprehensive assessment of the vulnerability of the source to contamination. This should obviously be done before any investment is made in construction.
The quality of the proposed source water should be tested under "worst case" conditions (those periods when contamination is most likely to occur such as the start of a wet period or when groundwater levels are raised) whenever possible. A sanitary inspection and pollution vulnerability assessment of the source should also be undertaken under "worst case" conditions.
If the source is contaminated, this may not preclude it's use as a source of drinking-water, as it may still be the best quality source available and/or the best source on other grounds such as cost, availability and quantity. Initial analysis should provide information on the nature of contaminants present and therefore an indication of what treatment processes will be required to remove them prior to distribution. A sanitary inspection should indicate the risk to the source from sources of microbiological contamination in the immediate surroundings of the source and suggest measures that may be taken to protect the source from continued contamination. A pollution vulnerability assessment will provide information on the risk to the source of contamination from a wider perspective and identify potential risk from chemical contamination.
Water source protection
Water source protection is a mixture of localised measures designed to protect individual sources and wider ranging measures designed to protect the larger water resource body. The latter can be on a provincial, national or regional (international) basis. For surface waters, the most appropriate level to protect water sources is though basin management. Depending on the size of the catchment area and water body, this may mean working on a scale ranging from district or provincial level up to international treaties involving several riparian countries (for instance the Nile and Zambezi basins).
As surface water sources and resources are far more open to contamination and potential catchment areas of contamination are generally far larger than for groundwater. Thus, any measures taken to protect surface water resources will generally encompass a far wider geographical region than measures designed to protect groundwater resources.
It is important that both localised and wider measures are undertaken to protect sources used for drinking-water supplies. Local measures are required to ensure that the actual water source is not at risk from contamination in its immediate environment. An example of this is well-head completion measures on the top of boreholes which ensure that the top of the borehole is sealed against the entry of contaminated surface water. Large-scale measures are required to ensure that valuable water sources are not lost because of contamination of the water body some distance away from the drinking-water source. An example of this is the definition of land-use zones around important aquifers to limit potential contamination.
Groundwater protection
Groundwater is an important source of drinking-water. In its natural state, groundwater is generally of high microbiological quality with little or no contamination, although some groundwaters do have high levels of harmful chemicals such as fluoride and arsenic. The relative purity of groundwater in its natural state is largely a result of infiltration through the soil and unsaturated layers of rock. During infiltration attenuative processes such as sorption, mechanical filtration and ion exchange operate which remove bacteria and some chemicals, particularly metals, from the water. However, some chemical compounds, such as nitrate, are not easily attenuated and once in the sub-surface aquatic environment are highly persistent and mobile. It is thus important that such chemicals are prevented from entering aquatic systems.
Once an aquifer is contaminated, as the movement of water through sub-surface systems relative to their volume is slow and residence times are lengthy, the natural processes of removal by dilution and discharge to surface waters may be extremely long (decades, centuries or millennium). Thus prevention of contamination of groundwaters by persistent mobile contaminants is an essential element in the protection of groundwater resources. A further complication is that many attenuative processes in the saturated zone are reversible and whilst initially contaminants may be removed from solution through, for instance sorption, at a later date they may be desorped and re-enter the water. This is a common problem in industrial cities in western Europe, where initial development led to a decrease in the water and subsequent attenuation of contaminants in the unsaturated zone. Subsequent development has occurred elsewhere using different water sources leading to a recovery of groundwater levels and desorption of contaminants and groundwater pollution. For instance there has been a noticeable increase in the levels of heavy metals in recovering groundwaters beneath London.
Different types of aquifers are vulnerable to contamination to differing degrees. Generally where aquifers are overlain by a substantial unsaturated zone and have high primary porosity and reasonable permeability, they tend to be less vulnerable to pollution. Aquifers where water is primarily held in secondary porosity (fissures and joints) tend to be more vulnerable to contamination as the water has less opportunity to undergo attenuative processes which remove contaminants.
This has led the concept of "Groundwater Protection Zones" where acceptable land uses are defined in order to protect the underlying groundwater. These zones were originally developed in Western Europe, particularly Germany and the Netherlands, to prevent contamination of groundwater supplies by pathogens and thus reduce the incidence of water borne diarrhoeal diseases. The delineation of groundwater protection zones is done by establishing the length of time a substance or organism takes to become non-harmful and the distance this represents under groundwater flow conditions.
Microbiological groundwater protection zone are established on the basis that the vast majority of pathogenic bacteria die off within 50 days of being in groundwater under normal conditions. Thus by establishing the distance travelled by groundwater in 50 days for a particular area, a zone can be defined from the abstraction point.
The definition of zones for chemical protection has also been attempted but this has been far less successful than the delineation of microbiological zones. This is because, unlike microbiological survival rates, it has proved extremely difficult to establish or even estimate the half-life of many chemicals in groundwater. Not only is there a vast number of chemical compounds which may be found in water, but groundwater and aquifers (particularly hard rock aquifers) frequently have a complicated chemistry themselves which may interact with pollutants and extend or reduce half-life. A 400-day isochron has been suggested in some quarters as being sufficient, but in reality far more work is needed in this area and chemical persistence will vary with different chemicals and aquifers.
Groundwater Protection Zones may take many shapes. They are very rarely simple circles drawn with an abstraction point as the centre. There are many factors which will influence the shape of the zone: the nature of the aquifer (which are very rarely isotropic); the number of rivers in the zone; the condition of rivers (whether influent, effluent, perched or changing); and the number and location of other abstraction points within the zone.
Surface waters which overlie an aquifer will extend the zone along its course upstream as contaminants are likely to move more quickly in surface water. It is important to establish what relationship the river bears to the aquifer, as obviously where a river is supplied by the aquifer the protection zone need not be as extended as when the river recharges the aquifer. However, it is always likely that a river will be influent to an aquifer at some point along its course. Even under effluent conditions there will be river-groundwater interaction and the extension of a zone some way along river which is recharged by the aquifer is always to be recommended. The more rivers associated with the aquifer, the greater the distortion and extension of the zone.
Within the protection zone, land use may be restricted to non-polluting activities and ensure that any discharges within the zone meet stringent quality standards. This may be problematic where there is intensive agriculture with widespread use of inorganic fertilisers and pesticides. In these cases, permitted application loads may be introduced and groundwater quality monitored. In these circumstances is often found that producers can reduce applications whilst maintaining yields, although it is possible that some form of compensation for loss of production may have to be provided. Where intensive animal production is practised, adequate isolation and treatment of slurries should be carried out by the farmer and leakage to groundwater minimised.
Surface Water Protection
Surface waters are particularly vulnerable to contamination from agricultural, industrial and municipal sources. Surface water bodies receive wastewater from industrial and municipal sources, agrochemicals may leach into them, air-borne pollutants may dissolve in surface water and they receive overland run-off which washes surface debris. As a result, all surface waters require treatment before they are supplied for drinking-water, whether the source is a river, lake or reservoir.
There are a number of interventions which will help to protect the quality of surface waters, principal amongst these are: land-use control within the catchment; and proper siting of intake structures away from potential sources of pollution and preferably upstream of them; treatment of effluent and discharges leaving industrial plants and municipal sewage treatment works, and; the establishment and enforcement of effluent quality standards.
Where surface water is used as a source of drinking-water, it is appropriate to ensure that land use within the catchment is controlled and preferably limited to activities which are relatively non-polluting. This can be problematic as some activities may already be established which do cause pollution and in these cases, adequate standards of effluent quality should be established and enforced.
Land-use control has tended to be more effective when applied to artificial reservoirs, principally because in many countries these have been located away from intensive human activity. However, land-use controls may be difficult to introduce as the creation of a large body of water may attract industry which will have effluent discharges. Reservoirs may promote intensive arable agriculture which utilises inorganic fertilisers and pesticides which may pollute the reservoir.
In many countries, standards have been or are being developed and enforced governing the quality of effluent that may be discharged into a river or standing body of water and in many countries, national bodies concerned with water are trying to shift the onus onto producers to treat wastewater prior to discharge - the 'polluter pays' principle. However, few countries have managed to enforce compliance with these standards and large-scale pollution continues. In many countries the penalties for exceeding quality standards are minimal and as the cost of installing treatment processes in the plant greatly exceed the accumulated cost of fines, there is little incentive for the producer to invest in treatment technology. This situation is often exacerbated by the time it takes for cases involving pollution to reach court, further reducing the real cost to the producer.
The rigorous enforcement of compliance with effluent quality standards backed up with adequate legislation which has penalties which reflect the severity of the pollution event will make a significant contribution to the improvement in surface water quality. However, positive influence should also be exerted to assist industry to employ discharge treatment in their plants. This may include awareness raising in the industry sector, technical advice concerning technology choice and may also involve other incentives to industry, such as tax breaks or subsidies, to promote the use of treatment of effluents.
Sediments in surface waters also interact with pollutants in the aquatic environment and can become "reservoirs" of pollution. Where chemical contaminants, particularly metals, are in water there are commonly ion exchange reactions with minerals in the sediment and diffusion of chemicals into the sediment which leads to contaminant build-up. Where there is significant organic material in sediments or the base of streams, metals form organic complexes. These processes may remove contaminants from the water in the short-term, but may be released back into the aquatic environment at a later date, usually in response to a specific flood event. Thus stopping a polluting activity will not lead automatically to a rapid reduction in contaminant concentration in surface waters.
Conclusion
Water source and water resources protection are essential if high quality waters are to remain uncontaminated. Both groundwaters and surface waters are vulnerable to pollution and both require localised and larger-scale actions to prevent pollution of drinking-water sources. Surface waters are open to more immediate pollution and once a pollutant enters a surface water body, it is likely to move rapidly. This means that the pollutant will spread rapidly through the surface aquatic system, although it may make remediation easier, except where there is significant water-sediment interchange.
Groundwater has more natural defences against pollution, however once it becomes polluted it is very difficult to remove the pollutant from the groundwater system and residence times of pollutants may be decades, centuries or longer. Different types of aquifer have differing degrees of vulnerability and thus have different protection requirements.
Both surface and groundwater resources are protected by defining land-use zones around them. This ensures that the establishment of potentially polluting activities is not allowed within a distance that would allow easy pollutant movement. Control of pollution is vital for water source and water resource protection and should be rigorously enforced.
References
Chilton, J., Groundwater, in Chapman. D., (ed) Water Quality Assessments (2nd edition), Chapman and Hall, London, 1996.
Environment Agency, Policy and Practice for the Protection of Groundwater, Environment Agency, London 1996.
Foster, S.S.D. and Hirata, R. Groundwater Pollution Risk Assessment, CEPIS, PAHO/WHO, Lima 1988.
Newson, M. Land, Water and Development, Routledge, London, 1992.
Presentation Plan
|
Section |
Key Points |
OHP |
|
Introduction |
· prevention of contamination is important and preferable to treatment |
1 |
| |
· this is achieved through: source protection; water resource management; good design and operation; and surveillance | |
| |
· source selection is important, always select best source available |
|
|
|
· sources should be assessed under worst case conditions |
|
|
|
· contaminated sources can still be used | |
|
Water Source Protection |
· mixture of localised and broader measures |
2 |
| |
· localised measures prevent contamination in immediate vicinity, sanitary completion measures | |
| |
· broad scale measures prevent pollution of water resources and loss of water sources from distant pollution | |
|
Groundwater Protection |
· natural state is very good microbiological quality |
3,4,5,6,7,8 |
| |
· chemical quality is sometimes less good | |
| |
· natural removal of contaminants through attenuative processes | |
| |
· once contaminated, removal is expensive and difficult | |
| |
· different aquifers have different vulnerabilities | |
| |
· groundwater protection zones define acceptable land uses around water sources to prevent contamination |
|
| |
· definition of zones for microbiological protection are easy, zones for chemical protection are more difficult | |
| |
· shapes of zones vary and surface water-groundwater interactions affect zone shapes and extent | |
|
Surface Water Protection |
· surface water is very vulnerable to contamination from many sources and pollutant move rapidly through surface water bodies |
9,10,11,12,13 |
| |
· surface water always requires treatment prior to consumption |
|
|
|
· sources protected through land use control, intake design and pollution control | |
| |
· land use in immediate upstream vicinity of source should be restricted to non-polluting activities | |
| |
· effluent control is important and stringent standards and end of pipe treatment are all required | |
| |
· legislative support and awareness raising in industry are important | |
|
Conclusions |
· need source and resource protection to maintain high quality waters | |
| |
· surface water is more vulnerable to pollution than groundwater | |
| |
· pollutants move rapidly in surface water and surface water always requires treatment | |
| |
· once contaminated, remedial action for groundwater is expensive and difficult | |
| |
· control of land use is important for both groundwater and surface water | |
Source Protection
· Prevention of contamination is preferable and more sustainable than treatment· Source selection is important
· Assess potential source of drinking-water under 'worst case' conditions
· Contaminated sources may still be used provided minimum treatment requirements are met
Source Protection Measures
· Localised:
sanitary well seal
protected intakes
· Large scale:
watershed management
groundwater protection zones
water resource management policies
Groundwater Definitions
Aquifer:
Rock or unconsolidated deposit containing water
Porosity:
The percentage of voids in a formation.
Permeability:
Measure of inter-connectedness of pores
Bulk permeability:
Flow through mass as a whole
Intrinsic permeability:
Rate at which rock will allow fluid to pass independent of fluid
Groundwater Protection Zones
· Zones for land use control to prevent contamination
· Based on contaminant persistence and travel time
· Very high flows - possibly reduce travel time as increase attenuation
50 DayIsochron:
· For control microbiological contamination
· Most microbes die within 50 days in groundwater
400 DayIsochron
· Used to control persistent chemicals
An alternative is 25 per cent of the recharge area
Source Catchment
· Protects the area of long-term annual recharge.

Organism Survival

Distance-time Curve
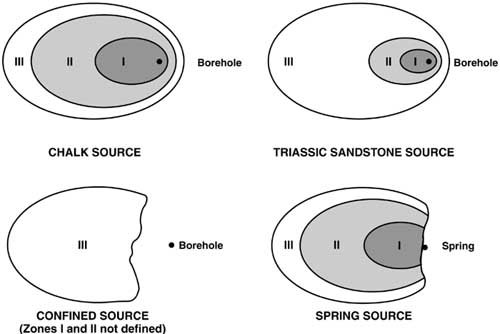
Examples of Protection Zones (NRA,
1992)

Simplified lithological
classification of geological formation in terms of relative risk of groundwater
pollution
Source: Foster, 1987
Protected River Intake

A. Plan view
B. Cross Section
Water Resources Protection
· Land use planning and control
· Environmental conservation and habitat protection
· Pollution control

Model of Issues and Activities in
Surface Water Management
Source: Newsom, 1994
Pollution Sources and Control
· Land-based diffuse:
land use control
control on agrochemical use
· Point source:
effluent quality standards
enforce compliance
· Air-borne particulate matter:
difficult to control
international treaties on air
pollution reduction

Impacts of Intermediate Reservoir
Storage in Hydrology and Water Quality
Source: Newsom, 1994
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Water Treatment
Session Objectives
· To demonstrate the need for treatment of surface waters and some groundwaters for drinking purposes.· To introduce the concept of the multiple barrier principle and to describe the more common and important key processes.
· To describe the function of each treatment process in treating drinking-water.
· To provide a basic outline on the selection of technology.
· The discuss the assessment of water treatment plants.
Introduction
All surface water and some groundwaters require treatment prior to consumption to ensure that they do not represent a health risk to the user. Health risks to consumers from poor quality water can be due to microbiological, chemical, physical or radioactive contamination.
However, microbiological contamination is generally the most important to human health as this leads to infectious diseases which affect all populations groups, many of which may cause epidemics and can be fatal. Chemical contamination, with the exception of a few substances such as cyanide and nitrate, tends to represent a more long-term health risk. An example of this is nitrate which can cause methaemoglobinaemenia in babies. Substances in water which affect the clarity, colour or taste of water may make water objectionable to consumers and hence ability to recover costs. As many microorganisms are found associated with particles in water, physical contamination may also represent a health risk as it extends microbial survival.
Most treatment systems are designed to remove microbiological contamination and those physical constituents which affect the acceptability or promote microorganism survival - largely related to the suspended solids in the water. A disinfectant is nearly always included in treatment plants of any size. This is done for two main reasons: firstly it is added to inactivate any remaining bacteria as the final unit of treatment; and, more importantly, to provide a residual disinfectant which will kill any bacteria introduced during storage and/or distribution.
The multiple barrier principle
Treatment processes usually function either through the physical removal of contaminants through filtration, settling (often aided by some form of chemical addition) or biological removal of microorganisms. It is usual for treatment to be in a number of stages, with initial pretreatment by settling or pre-filtration through coarse media, sand filtration (rapid or slow) followed by chlorination. This is called the multiple barrier principle.
This is an important concept as it provides the basis of comprehensive treatment of water and provides a system to prevent complete treatment failure due to a breakdown of a single process. For instance, with a system which comprises addition of coagulation-flocculation-settling, followed by rapid sand filtration with terminal disinfection, failure of the rapid sand filter does not mean that untreated water will be supplied. The coagulation-flocculation-settling process will remove a great deal of the suspended particles, and therefore many of the microorganisms in the water, and the terminal disinfection will remove many of the remainder. Provided the rapid sand filter is repaired reasonable quickly, there should be little decrease in water quality.
A key element in the multiple barrier principle is to ensure that the source of water is protected and maintained at as high a quality as possible. This is sometimes easier for groundwater sources on a local scale, although there are obvious difficulties for both ground and surface water on a larger scale.
Treatment processes - advantages and disadvantages
There are many different treatment process available and whose suitability is a function of the source water quality, level of operator training and resources available for operation and maintenance. It is imperative that the selection of technology for treatment plants is done taking the above into consideration to ensure that they remain sustainable.
Prefiltration
As many secondary filtration processes, and in particular slow sand filtration, require low influent turbidities, some form of pretreatment to reduce suspended solids load is required. One way to achieve this is by using prefiltration of water through coarse media, usually gravel or coarse sand. Prefilters can have many different configurations: horizontal; vertical upflow; and vertical upflow-downflow. Vertical prefilters have become increasingly popular as they require far less land than horizontal prefilters and can take faster flow runs through them. An alternative are pressure filters, through which water is pumped at pressure to remove the suspended solids load.
Prefilters have an advantage in that they do not require chemicals, have limited working parts and are robust. They do however, require frequent cleaning and maintenance and are ineffective in removing fine particles, thus where the suspended solid load is primarily made up of silt and clay particles prefiltration is ineffective. Prefiltration is a physical process designed to remove suspended solids and therefore it's efficiency in removal of microorganisms is a function of the microbes associated with particles. Virus removal is poor and prefiltration is not effective in the removal of cysts or bacteria associated with fine particles.
Sedimentation
Sedimentation is the removal of suspended solids through the settling of particles moving through a tank at a slow rate. There are a number of forms of sedimentation. In water treatment plants treating source water a high proportion of suspended solids of coarser grades (e.g. sand and coarse silt) a grit chamber may be used to remove the largest particles through simple sedimentation. In this process, water is passed through a tank at a slow rate and suspended solids fall out of suspension. In small supplies, simple sedimentors may also be used, which functioning in a similar fashion to grit chambers, although with a slower rate of water throughflow. Simple sedimentation will not remove fine grained particles because the flow rates remain too high and the retention time is insufficient. A further common fault with simple sedimenters is that design flow rates are rarely achieved in practice and a certain element of 'short-circuiting' can occur unless construction, operation and maintenance is very careful.
As a result of the drawbacks in simple sedimentation, it is common to find that the sedimentation process is enhanced through the addition of chemicals - or coagulation. Coagulants carry a charge and therefore attract charged clay particles. The particles begin to aggregate and form 'flocs'. Once the flocs reach a critical mass, they sink to the bottom of the settler. The outlet of the sedimenter is generally around the top of the structure, thus the clear water is removed by a surface channel. This system can be further refined with the use of modular or plate settlers which reduces the time require for settling by providing a wider surface area for aggregation of particles.
The most commonly used coagulants is aluminium sulphate, although there are other coagulants available including ferric salts (sulphates and chlorides) and polyelectrolytes. Coagulants are dosed in solution at a rate determined by raw water quality near the inlet of a mixing tank or flocculator. It is essential that the coagulant is rapidly and thoroughly mixed on dosing, this is may be achieved through the use of a hydraulic jump. The water then passes into the settler to allow aggregation of the flocs. Increasing use is now being made of synthetic polymer compounds or polyelectrolytes. As these are highly charged, there is a rapid increase in the formation of flocs, particularly where clay makes up a large proportion of the suspended solid load.
The advantages of the coagulation is that it reduces the time required to settle out suspended solids and is very effective in removing fine particles which are otherwise very difficult to remove from water. Coagulation can also be effective in removing protozoa, bacteria and viruses, particularly when polyelectrolyte is used, as the highly charged coagulant attracts the charged microorganisms into the flocs. Coagulation can also be effective in removing by precipitation certain contaminants such as lead and barium.
The principle disadvantages of using coagulants are the cost and the need for accurate dosing, jar testing and dose adjustment and frequent monitoring. Coagulants can be expensive to buy (particularly polyelectrolyte) and need accurate dosing equipment to function efficiently. Staff need to be adequately trained to carry out jar tests to determine coagulant dosage.
Sand Filtration
Sand filtration can be either rapid or slow. The difference between the two is not a simple matter of the speed of filtration, but in the underlying concept of the treatment process. Slow sand filtration is essentially a biological process whereas rapid sand filtration is a physical treatment process.
Slow sand filters have an advantage over rapid sand filters in that they produce microbiologically "clean" water which should not require disinfection to inactivate any bacteria, although the addition of a disinfectant to provide a residual for the distribution system is still advisable. However, because of their slow flow rate, slow sand filters require large tracts of land if they are to supply large populations and can be relatively labour intensive to operate and maintain. As the reestablishment of the schumtzdecke takes several days, the plant has to have sufficient capacity to supply the water demand when one or more filters are out of action.
Rapid sand filtration is now commonly used worldwide and is far more popular than slow sand filtration. The principal factor in this decision has been the smaller land requirement for rapid sand filters and lower labour costs. However, rapid sand filters do not produce water of the same quality as slow sand filters and a far greater reliance is placed on disinfection to inactivate bacteria. It is also worth noting that rapid sand filters are not effective in removing viruses.
Slow sand filters
Slow sand filters operate at slow flow rates, 0.1 - 0.3 metres per hour. The top layers of the sand become biologically active by the establishment of a microbial community on the top layer of the sand substrate. These microbes usually come from the source water and establish a community within a matter of a few days. The fine sand and slow filtration rate facilitate the establishment of this microbial community. The majority of the community are predatory bacteria who feed on water-borne microbes passing through the filter.
The microbial community forms a layer called the schumtzdecke and can develop up to 2cm thick before the filter requires cleaning. Once the schumtzdecke becomes too thick and the rate of filtration declines further it is scraped off, a process done every couple of months or so depending on the source water. Once this has been carried out, the slow sand filter will not be fully functional for another 3 to 4 days until a new schumtzdecke has developed, although this procedure can be speeded up by seeding the filter with bacteria from the removed schumtzdecke. Slow sand filtration is extremely good at removing microbial contamination and will usually have no indicator bacteria present at the outlet. Slow sand filters are also effective in removing protozoa and viruses.
Slow sand filters require low influent turbidity, below 20TU and preferably below 10TU. This means that efficient pretreatment is required to ensure that the filters do not become overloaded. Slow sand filters can cope with shock turbidities of up to 50TU, but only for very short periods of time before they block. The sand used in slow sand filters is fine, thus high turbidities cause the bed to block rapidly and necessitates more frequent cleaning and therefore greater time out of action. Nevertheless, slow sand filters are still used in London and were relatively common in Western Europe until comparatively recently and are still common elsewhere in the world. The move away from slow sand filtration has largely been a function of rising land prices and labour costs which increased the cost of slow sand filter produced water, where this is not the case, slow sand filters still represent a cost-effective method of water treatment.
Rapid sand filters
Rapid sand filters work at much higher rates of flow (up to 20 meters per hour) and essentially rely on physical removal of suspended solids, including any floc carried over from the settlers. Although rapid sand filters achieve some reduction in microbial populations in water as it removes particles to which bacteria are attached, it is not a biological treatment and the use of a terminal disinfectant is vital to ensure that bacteria in the water have been inactivated. Rapid sand filters require frequent cleaning (daily or twice daily) which is achieved through backwashing filters with clean water to re-suspended the sediment. Cleaning takes relatively little time and the filters can be put back into operation immediately.
Rapid sand filters are far smaller than slow sand filters and are commonly employed in 'batteries'. The rapid flow rate through these filters means that demand can be more easily met from smaller plants. Rapid sand filters do not require low influent turbidities, as they are essentially a physical treatment process, although higher suspended solids loads will result in more frequent cleaning. Backwashing is usually rapid and filters are not out of commission for mare than a matter of minutes. Cleaning and operation can be largely mechanised and air scour is commonly employed to make backwashing more effective. With the small land requirement, several rapid sand filters can be accommodated in small area and thus it is easy to maintain capacity to meet demand when filters are being cleaned.
Disinfection
Only a very brief discussion of disinfection is included here for completeness sake and for further information please refer to session XIV of the Teaching Pack or to Chapter 6 of Volume 1 of the Guidelines and Chapter 6 of Volume 3.
All water supplies should be disinfected in order to protect public health. Disinfection inactivates any remaining bacteria in the water after previous treatment steps and provides a residual disinfectant to inactivate bacteria introduced by any subsequent ingress of contaminated water during storage or distribution.
At present, the principal disinfectant used worldwide is chlorine, although alternatives are being increasingly investigated and process such as ozonation are becoming more important in industrialized countries. It is important to note that all disinfectants produce by-products and that the greater knowledge about the by-products formed from the use of chlorine because it is this most widely used disinfectant should not compromise it's use. It is also important that disinfection of water supplies is never compromised because of a risk of potential health effects from by-products in the final water. Any health impacts from chemical contamination is likely to be long-term, whereas the absence of disinfection puts the consumers at risk from infectious diarrhoeal disease.
Other Treatment Processes
The above treatment process are all designed to make drinking-water safe by the removal of microorganisms and suspended solids. However, drinking-water, particularly from groundwater sources, may also contain chemical contaminants which must be removed. Generally the removal of chemicals from water is more difficult and much more expensive than removing microbiological or physical contaminants. Basic filtration and coagulation techniques are not generally effective for the majority of chemicals.
As there are many different chemicals which could be dealt with, a few relevant examples will be provided. Iron can be a major constituent of both ground and surface waters (where it is commonly associated with bacteria and algae). Although iron does not represent any health risk, it causes problems of acceptability of the water as many consumers find the colour off-putting and because it stains clothes. The principal method of removing iron from water is through aeration or oxidation of the Fe2+ to the Fe3+ species. This is easily achieved by flowing the water over a simple cascade and followed by sedimentation. Note aeration is also used for waters known to be anoxic or oxygen deficient.
A variety of processes are used for the removal of organic and inorganic contaminants including ion exchange and precipitation. For instance, fluoride may be removed through coagulation with lime or by ion exchange using calcinated burnt bone or activate alumina. Granulated activated carbon (GAC) is commonly used for pesticide removal through adsorption. This is expensive but unfortunately no other process appears to work effectively and therefore GAC remains the sole option.
Selecting Technology
When selecting technology and systems of treatment it is vital that as full a picture as possible of the source water quality is available. It is important to know what is in the water before trying to design appropriate treatment systems. It is equally important to maintain a thorough monitoring programme through the plant to ensure that each stage of treatment is working effectively and efficiently.
All waters may need treatment before they are fit for human consumption, although surface waters tend to be more vulnerable to contamination than groundwater. All surface waters will require treatment prior to consumption. Furthermore, all water supplied through distribution systems should be disinfected to provide a residual disinfectant which provides ongoing protection from bacterial growth and survival.
Presentation Plan
|
Section |
Key points |
OHP |
|
Introduction |
· need to treat all surface waters and some groundwaters |
|
|
|
· contamination may be microbiological, chemical or physical | |
| |
· microbiological contamination is most important as it causes highly infectious disease with short-term impacts | |
| |
· chemical contamination tends to have longer term effects on health | |
| |
· suspended solids affect microbial survival and the acceptability of water | |
| |
· always disinfect water supplies and maintain a residual in the water for protection against contamination during distribution and storage | |
|
Multiple Barrier Principle |
· need to have more than a single process during treatment |
1 |
| |
· prevents breakdown in one process leading to complete treatment failure | |
| |
· source must be well protected | |
|
Treatment processes |
· many processes available, the suitability of each is a function of source quality, operator capacity and financial resources |
2,3,4,5 |
| |
· technology selection must be made on the basis of the above to ensure sustainability | |
| |
· often need to reduce turbidity before treating water as this may interfere with treatment | |
| |
· prefiltration is a physical process which removes suspended solids | |
| |
· prefilters can be horizontal, vertical upflow or vertical upflow-downflow | |
| |
· main advantage is limited working parts and doesn't use chemicals | |
| |
· disadvantages include poor ability to remove fine material, microbial removal poor and may need frequent cleaning | |
| |
· sedimentation is achieved by the settling of particles in slow moving water | |
| |
· simple sedimenters do not use chemical coagulants and are not effective in removing fine material | |
| |
· settling is improved through addition of coagulants to form larger aggregates which speeds up settling and removes fine material | |
| |
· modular and plate settlers improve settling efficiency |
|
|
|
· alum is the most common coagulant, others include polyelectrolytes and ferric salts such as sulphate and chloride | |
| |
· advantages include removal of fine particles, removal of some viruses, quick, compact | |
| |
· disadvantages include expense, need for good monitoring capacity, need trained operators | |
|
Treatment processes |
· sand filtration can be rapid or slow |
6,7 |
| |
· slow sand filtration is a biological process and rapid sand filtration a physical process | |
| |
· slow sand filters a biologically active top layer called the schumtzdecke which is composed of predatory bacteria | |
| |
· schumtzdecke kills bacteria and viruses | |
| |
· require cleaning at every 2 months, take 3-4 days to recover |
|
|
|
· rapid sand filters work at much faster rates and remove suspended solids | |
| |
· advantages of slow sand filtration include production of good quality water, relatively simple to operate | |
| |
· disadvantages include large land requirement, labour intensive, requires low turbidity water | |
| |
· advantages of rapid sand filtration include small land requirement | |
|
Treatment plant assessments |
· assessments of treatment plants may be carried out for a number of different reasons |
8,9 |
| |
· routine assessments often carried out by water suppliers to ensure performance is efficient and optimised | |
| |
· assessments may also be undertaken when there is a failure in water quality or a failure to produce water of adequate quality | |
| |
· assessments involve the evaluation of each unit process to ensure that it performs efficiently and to identify any process failures and causes of failures | |
| |
· assessments should also evaluate the suitability of combinations of technologies (e.g. sometimes find simple sedimenters combined with slow sand filters when turbidity was relatively high - led to failure) | |
| |
· assessments should be linked to performance optimisation |
|
|
Conclusion |
· both surface and groundwater may require treatment before distribution | |
| |
· source water quality (and likely variations) should be known before selecting technologies | |
| |
· technologies should be used which reflect capacity to operate the plant and which provide adequate treatment | |
| |
· a multiple barrier principle should always be used when treating water | |
| |
· source protection is also vital | |
NB: OHPs 8 and 9 may be used when discussing water treatment plant monitoring and assessment
The Multiple Barrier Principle of
Water Treatment
Upflow-Downflow Prefilter
Horizontal Flow Prefilter
Flocculator
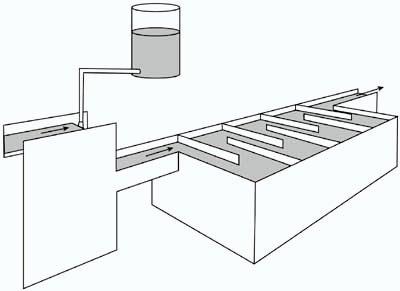
Coagulant Dosing
Slow Sand Filter
Rapid Sand Filter
Water Treatment Plant Assessments
When and why the should be carried out:
· Routine assessment of operational efficiency and state of equipment
· When contamination is found
· When disease outbreaks occur
· If disinfection dosing requirements suddenly change
Water Treatment Plant Assessments Parameters
Raw Water:
turbidity, pH, alkalinity, coliforms, major ions, nutrients, known problem substances
Coagulation-flocculation-settling:
turbidity, pH, residualaluminum, residual acrylamide, coliforms
Prefiltration:
turbidity, pH, coliforms
Sand filtration (rapid/slow):
turbidity, pH, coliforms
Disinfection:
residual (usually chlorine), pH, turbidity, coliforms (thermotolerant and total)
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Disinfection
Session Objectives
· To introduce the principal disinfectants that may be used and highlight key advantages and disadvantages of each· To emphasise the use of chlorination for routine disinfection.
· To describe the process of chlorination and discuss the concepts of breakpoint chlorination, chlorine demand and outline basic chlorine chemistry.
· To discuss the types of chlorine available and how these may be used for routine disinfection.
Introduction
All water supplies should be disinfected. This is aimed both at inactivating remaining bacteria before distribution and providing a residual disinfectant to inactivate bacteria introduced by any subsequent ingress of contaminated water during storage or distribution. At present, the principal disinfectant used worldwide is chlorine, although alternatives are being increasingly investigated and process such as ozonation are becoming more common.
Chlorine is generally the disinfectant of choice as it is reasonably efficient, cheap and easy to handle. In all but the smallest water treatment plants, chlorine is added to water as either in aqueous solution (calcium hypochlorite or sodium hypochlorite) or chlorine gas. Smaller supplies may use tablets of hypochlorite.
Other disinfectants include ozone, ultraviolet light and iodine. These all have disadvantages. UV is not a particularly effective disinfectant and it is difficult to expose water for sufficient time for disinfection to be effective. Neither ozone or UV provide a residual disinfectant and therefore offer no protection against recontamination in distribution. To overcome this, in some water supplies booster ozonation stations are set up along the distribution network.
Both iodine and ozone are carcinogenic. There are also significant health and safety concerns, for operators, regarding the generation and application of ozone and chlorine (especially in the gaseous form). Iodine can also lead to thyroid problems with pregnant women and is generally more toxic than chlorine.
Selection of disinfectant
Under most circumstances, overwhelming factors will dictate selection of disinfection method. The most common major factors are: availability, cost of disinfectant, logistics (especially transport costs), and cost/availability of equipment. Under the majority of circumstances chlorine in one of its forms has been found to be the disinfectant of choice. The choice of which form of chlorine will again largely be determined by availability, cost and transport.
Chlorine
Chlorine is an effective disinfectant where water is not turbid (cloudy) and the pH of the water to be treated is not alkaline, for instance not above pH 8.0. However, most natural waters have a pH below 8.0 and thus disinfection is rarely compromised by pH.
Chlorine chemistry
Chlorine, whether in the form of pure chlorine gas from a cylinder, sodium hypochlorite or calcium hypochlorite in any of its presentations, dissolves in water to form hypochlorous and hydrochloric acids. Chlorine dioxide, however, does not dissolve in water.
The reaction of chlorine in water follows the reaction shown below:
Cl2 + H2O ® HOCl + HCl
Hydrochloric acid dissociates in turn to form hydrogen and chloride ions
HCl ® H+ + Cl-
Hypochlorous acid however dissociates only partially
HOCl Û H+ + OCl-
It is undissociated hypochlorous acid which acts as a disinfectant. The equilibrium between undissociated hypochlorous acid, hydrogen ions and hypochlorite ions depends on pH. At high pH (alkaline conditions, pH greater than 8), the dissociated forms predominate and at low pH (acidic conditions) undissociated hypochlorous acid predominates. For this reason disinfection with chlorine is more efficient at lower pH values and a pH of less than 8 is recommended for disinfection. Pure chlorine gas from a cylinder tends to decrease the pH of the water slightly; hypochlorite tends to increase water pH a little.
Formation of combined chlorine is due to a sequence of reactions. Hydrogen in ammonia is progressively replaced by chlorine as follows:
|
NH3 |
® |
NHCl |
® |
NHCl2 |
® |
NCl3 |
|
ammonia | |
monochloramine |
|
dichloramine |
|
nitrogen trichloride |
Where it is desired to produce monochloramine as a more stable, but less efficient disinfectant, the two chemicals may be dosed in appropriate proportions.
NH3 + Cl2 = NH2Cl + HCl
If a large chlorine dose is applied (relative to ammonia), as is practised in breakpoint chlorination, then nitrogen is formed.
2NH2Cl + Cl2 ® N2 + 4HCl
Chlorine demand
The total amount of chlorine which will react with both compounds like iron and manganese and with organics and ammonia is referred to as the chlorine demand. The chlorine demand of different waters can vary widely.
Chlorine demand is the difference between the amount of chlorine added to the water (the chlorine dose) and the total chlorine detectable in the water. The chlorine demand for some waters, for instance some river waters, can increase dramatically, particularly after heavy rain.
Breakpoint chlorination
The type of chlorine dosing normally applied to piped water supply systems is referred to as breakpoint chlorination. Sufficient chlorine is added to satisfy all of the chlorine demand and then sufficient extra chlorine is added for the purposes of disinfection. Figure 1 shows the breakpoint chlorination curve. It indicates the effect of adding more chlorine to water which contains an initial ammonia nitrogen content of 1 mg/l.
Figure 1. Breakpoint chlorination.
Diagram taken from Tebbutt T.H.Y., 1992
The initial rise in residual is predominantly monochloramine (combined chlorine residual). The subsequent fall with further addition of chlorine is due to the decomposition of monochloramine to form nitrogen (the chlorine detected in this phase is also combined residual).
Finally the oxidation of ammonia is complete and any additional chlorine will cause an equal increase in the free chlorine residual.
Contact time
Disinfection with chlorine is not instantaneous. Time is required in order that any pathogens present in the water are inactivated.
The time taken for different types of microbes to be killed varies widely. In general, amoebic cysts are very resistant and require most exposure. Bacteria, including free-living Vibrio cholerae are rapidly inactivated by free chlorine under normal conditions. For example, a chlorine residual of 1mg/l after 30 minutes will kill schistosomiasis cercariae, while 2mg/l after 30 minutes may be required to kill amoebic cysts. Thus it is important to ensure that adequate contact time is available before water enters a distribution system or is collected for use.
Contact time in piped supplies is normally assured by passing the water, after addition of chlorine, into a tank from which it is then abstracted. In small community supplies this is often the storage reservoir (storage tank). In larger systems purpose-built tanks with baffles may be used. These have the advantage that they are less prone to "short circuiting" than simple tanks.
The pH of the water also affects the efficiency of chlorination and contact time is therefore also related to pH.
Chlorine residual
Chlorine persists in water as 'residual' chlorine after dosing and this helps to minimize the effects of re-contamination by inactivating microbes which may enter the water supply after chlorination. It is important to take this into account when estimating requirements for chlorination to ensure residual chlorine is always present.
The level of chlorine residual required varies with type of water supply and local conditions. In water supplies which are chlorinated there should always be a minimum of 0.5 mg/l residual chlorine after 30 minutes contact time in water.
Where there is a risk of cholera or an outbreak has occurred the following chlorine residuals should be maintained:
|
· At all points in a piped supply |
0.5mg/l |
|
· At standposts and wells |
1.0mg/l |
|
· In tanker trucks, at filling |
2.0mg/l |
In areas where there is little risk of a cholera outbreak, there should be a chlorine residual of 0.2 to 0.5 mg/l at all points in the supply. This means that a chlorine residual of about 1mg/l when water leaves the treatment plant is needed.
Problems of taste and odour
The taste of chlorine in drinking water may lead the population to reject a source of water which is actually safe to drink. They may then choose to use a better-tasting source of water which may in fact present a greater health risk. Chlorinous tastes in water are most often due to over-dosing or the presence of chlor-phenols.
Over-dosing may be due to error (which should be prevented by proper monitoring and control); may be deliberate (for instance, in response to contamination of the supply, which should be corrected as soon as possible and chlorine levels returned to normal); or may be due to high-level dosing to ensure adequate concentrations in remote parts of the distribution network (in this case consideration should be given to re-chlorination during distribution).
Chlor-phenols are formed where chlorine reacts with phenolic substances in water. These may be derived from algae, thus chlor-phenol formation is more common where the source is surface water than when groundwater sources are used. Chlor-phenols have a very strong chlorinous taste and very small amounts of chlorine can therefore give rise to very strong tastes. Problems with chlor-phenols are often transient and are best overcome by improving the intake and source.
Although chlorine itself can give rise to problems of taste and odour, chlorination can also help to improve taste and odour by the reduction of organic materials and iron.
As disinfection with chlorine is less effective in turbid water, water to be chlorinated should be clarified. This can be done by natural filtration as is the case with groundwater from wells and springs, or by filtration during water treatment. Filtration should also remove the cysts and eggs of protozoa and helminths which are resistant to chlorine.
Types of chlorine
Chlorine is available in various forms, including calcium hypochlorite, sodium hypochlorite and as pure chlorine gas in cylinders.
Calcium hypochlorite (chlorinated lime, tropical bleach, bleaching powder, 'HTH') is a powder containing between 30 and 70 per cent available chlorine. It must be stored carefully to prevent deterioration, and although it can cause burns, is generally safe to handle and transport. The Capital (equipment) costs of using calcium hypochlorite for disinfection are generally low. Calcium hypochlorite is most commonly used in solution for the disinfection of rural and small community water supplies and in diffusion hypochlorinators or in tablet form for household use.
Sodium hypochlorite (including household bleaches) is a solution. Sodium hypochlorite solutions contain about 1 to 18 per cent chlorine and are thus mostly water. The solution must be stored carefully to prevent deterioration, it can cause burns and is inefficient to transport, since it is mostly water. Sodium hypochlorite is most commonly used for disinfection in the home and in water supplies where transport of the solution is not a problem.
Pure chlorine gas in cylinders, is used widely. Specialized transport, handling and dosing equipment are needed. However, as chlorine in cylinders is not normally subject to deterioration it is an efficient means of storing and dosing chlorine. Leaks of chlorine gas are very dangerous and installations storing cylinders should be well designed, monitored and maintained. Chlorine in cylinders is most commonly used for dosing at water treatment plants, at the head of wells from which water is mechanically pumped and at re-chlorination plants in large distribution networks.
For more detail on the technologies of chlorination please refer to Volume 3 of the Guidelines.
Chlorine dioxide
Chlorine dioxide is a more powerful oxidizing agent than chlorine, the disinfectant action of which is less pH-dependent than chlorine. It leaves a long-lasting residual. However, chlorine dioxide is an inefficient disinfectant for viral agents and therefore its use is limited.
Chlorine dioxide is mainly used for the control of tastes and odours. It does not combine with ammonia to a significant extent and therefore is more efficient than chlorine in waters with raised levels of ammonia.
Chlorine dioxide is unstable and must be generated on-site by the action of chlorine or an acid on sodium chlorite. In general the two chemicals are dosed together into the water; this process requires constant, vigilant monitoring and control. Chlorine dioxide is much more expensive than chlorine.
Iodine
Where water is not turbid, iodine is an effective disinfectant and is more stable than chlorine in storage. Iodine is mostly used for disinfecting small volumes of water for personal use. It is generally too costly for dosing into community water supplies. Iodine reacts less with organic matter than chlorine and does not react with ammonia.
A dose of two drops of a 2 percent solution of iodine in ethanol, per litre of clear water has been recommended for disinfecting small volumes of water for personal use. However, 1-2 mg/l with a contact time of not less than 30 minutes is normally recommended for public water supplies. Most people begin to detect the taste and odour of iodine at concentrations in the range 1-2 mg/l.
Iodine in solid form is easy to store and deteriorates less rapidly than chlorine. If dissolved in ethanol however, iodine will deteriorate rapidly. Stable iodine compounds for dosing into water supply systems, such as tetraglycine potassium tri-iodide are available as tablets.
Iodine is rarely appropriate as disinfectant for long-term use in community water supplies, especially because of its cost. Nevertheless, because of its stability and effectiveness, it is very useful for disinfection of drinking water, especially in small volumes in emergency, or disaster situations.
At high doses (for instance above 4 mg/l) iodine may produce allergic reactions in some individuals and doubts exist regarding the advisability of long-term use of iodine for drinking water disinfection.
Ozone
Ozone (O3) is an unstable gas which is only slightly soluble in water. It is an efficient disinfectant, but because it is unstable does not leave a residual in water unlike chlorine. For this reason it is effectively impossible to over-dose with ozone. Ozone contributes to the bleaching of colour and removal of tastes and odours.
Ozone is produced by passing dry oxygen or air through an electrical discharge. It is manufactured on-site using specialized equipment. Whilst ozone is overall the most effective disinfectant and is more effective than chlorine in inactivating cryptosporidium oocysts and viral agents, there are significant disadvantages in its use. These are primarily that ozone does not provide residual protection against recontamination during distribution and as ozone affects biological stability, it may encourage regrowth of bacteria.
However, given the concerns about the use of chlorine in many countries, the use of ozone is increasingly investigated and the lack of residual may be dealt with by employing regular booster ozonation during distribution. However, far less is known about ozonation and the effect of ozone of human health and it should be remembered that ozonation is much more expensive than chlorination.
Ultraviolet radiation
Ultraviolet (UV) radiation has been used fairly extensively for disinfection of small community water supplies.
The efficiency of UV disinfection is dependent on the intensity and wavelength of the irradiation and the exposure of the microorganisms to the radiation. UV radiation therefore decreases in efficiency as contamination (especially turbidity and some substances in solution such as iron and organic compounds) increases.
UV disinfection of water is normally achieved by passing the water through tubes lined with UV lamps. This gives efficient disinfection after a contact time of a few seconds. A typical power requirement would be within the range 10-20 W/m3h. The lamps used disinfect using a wavelength of light around 254nm. The lamps may continue to produce blue light when they are worn out and no longer produce disinfecting irradiation.
Disinfection with UV irradiation does not give rise to tastes and odours. There is no requirement for consumable chemicals, maintenance is straight forward and there is no danger of over-dosing. UV irradiation does not leave a residual effect in the water. The equipment and consumables are expensive and water to be treated must be of consistently high clarity.
References
Anon. (1989) Disinfection of Rural and Small Community Water Supplies: a manual for design and operation. Water Research Centre. Medmenham, England.
Anon (1996) Guidelines for Drinking Water Quality Volume III - 2nd edition. World Health Organization. Geneva.
Tebbut, T.H.Y. (1992) Principles of Water Quality Control. 4th edition. Pergamon. Oxford.
Disinfectants and Disinfectant By-Products
Table 1: Summary of C.t values (mg/L. min) for 99% inactivation at 5°C (Clark et al, 1993)
|
Organism |
Disinfectant | |||
| |
Free chlorine, pH 6 to 7 |
Pre-formed chloramine, pH 8 to 9 |
Chlorine dioxide, pH 6 to 7 |
Ozone, pH 6 to 7 |
|
E. coli |
0.034-0.05 |
95-180 |
0.4-0.75 |
0.02 |
|
Polio virus 1 |
1.1-2.5 |
768-3740 |
0.2-6.7 |
0.1-0.2 |
|
Rotavirus |
0.01-0.05 |
3806-6476 |
0.2-2.1 |
0.006-0.06 |
|
Bacteriophage f2 |
0.08-0.18 |
- |
- |
- |
|
G. lamblia cysts |
47->150 |
- |
- |
0.5-0.6 |
|
G. muris cysts |
30-630 |
- |
7.2-18.5 |
1.8-2.0a |
|
C. parvum |
7200b |
7200c |
78b |
5-10c |
a Values for 99.9% inactivation at pH 6-9.
b 99% inactivation at pH 7 and 25°C.
c 90% inactivation at pH 7 and 25°C.
Presentation Plan
|
Section |
Key points |
OHP |
|
Introduction |
· all water supplies should ideally be disinfected to inactivate any |
OHP 1 |
| |
· pathogens in the water and to provide residual protection |
|
|
|
· a wide range of disinfectants have been evaluated in the GDWQ |
|
|
|
· principal disinfectant used world-wide is chlorine, although other | |
| |
· disinfectants such as ozone are also used | |
| |
· chlorinating involves addition of chlorine to water and although there are some health concerns about the use of chlorine, it is generally the disinfectant of choice | |
| |
· other disinfectants include ozone, ultraviolet and iodine |
|
|
|
· neither ozone or UV provide a residual and both iodine and ozone are carcinogenic | |
| |
· ozone is principal alternative to chlorine, however it does not provide residual protection and affects biological stability possibly increasing the risk of re-growth of bacteria |
|
|
Selection of disinfectant - Chlorine |
· chlorine is effective provided water is not turbid and the pH is below 8 |
2,3,4,5 |
| |
chlorine chemistry | |
| |
· chlorine dissolves in water to form hypochlorite ion and hypochlorous acid | |
| |
· hypochloric acid dissociates, but hypochlorous acid only partially dissociates | |
| |
· disinfectant is undissociated hypochlorous acid; at high pH dissociated forms predominate and this reduces efficiency | |
| |
· as tends to increase pH and hypochlorite decreases pH; it is important that the pH remains below 8 | |
| |
· chlorine reacts with ammonia to form amine compounds - nitrogen is formed during breakpoint chlorination | |
| |
chlorine demand | |
| |
· the total amount of chlorine in water which reacts with other compounds | |
| |
· chlorine demand varies considerably and is the difference between amount of chlorine added to water and free residual detectable in water |
|
|
|
breakpoint chlorination | |
| |
· this is the usual method of chlorination | |
| |
· sufficient chlorine is added to satisfy the chlorine demand, then extra chlorine added to provide a residual | |
| |
· initial rise of breakpoint curve is due to monochloramine formation; subsequent fall is due to decomposition of monochloramine to form nitrogen | |
| |
· once oxidation of ammonia complete, any additional chlorine leads to an increase in free residual | |
| |
contact time |
|
|
|
· disinfection with chlorine is not instantaneous | |
| |
· different microbes take different length of time to be inactivated by chlorine, therefore need an adequate contact time; this is usually 30 minutes | |
| |
· contact time is usually assured by passing piped water through a tank | |
| |
· contact time is also related to pH | |
| |
chlorine residual | |
| |
· residual is required to provide protection against recontamination | |
| |
· level of residual depends on water supply and local conditions |
|
|
|
· there should be 0.5 mg/l free chlorine after 30 minutes contact time | |
| |
· during outbreaks residuals should be maintained as follows: 0.5 mg/l all points in the supply; 1.0 mg/l at standposts and wells; 2.0 mg/l in tanker trucks at filling | |
| |
taste and odour problems | |
| |
· chlorine tastes may cause rejection of water supplies by consumers | |
| |
· bad tastes generally caused by over-dosing or presence of chlor phenols | |
| |
· over-dosing may be through error (easy to rectify); | |
| |
· over-dosing may be deliberate because contamination of supply (cause should identified and remedial action taken); or to ensure residual maintained at remote ends (consider booster chlorination) | |
| |
· chlor-phenols caused by reaction with phenolic substances, often derived from algae, therefore surface water more likely to give problems than groundwater | |
| |
· chlor-phenols have strong taste and should improve intake and source to reduce formation | |
| |
· chlorine can also improve taste by reduction on organics and iron | |
|
Types of chlorine |
· chlorine comes in various forms |
6 |
| |
calcium hypochlorite | |
| |
· powder containing 30-70% available chlorine; capital costs are low and commonly used for rural and household disinfection | |
| |
sodium hypochlorite | |
| |
· solution containing 1-18% available chlorine, used for household disinfection | |
| |
gaseous chlorine | |
| |
· pure chlorine gas and most effective and efficient form of chlorine | |
| |
· storage is important and safety measures must be in place |
|
|
Chlorination approaches |
· in piped water supplies chlorine is added to ensure that any microbes in water leaving the source/treatment plant are inactivated and to provide a residual protection for the distribution system |
7,8,9,10,11 |
| |
· under usual circumstances always maintain 0.2-.5 mg/l free chlorine residual | |
| |
· during epidemics or risk of epidemics, residual should be 0.5 mg/l at all points in pipe and 1mg/l at standposts | |
| |
· in point water sources, usually only disinfect during an epidemic or where risk of epidemic great |
|
| |
· residual should be 1 mg/l at all times | |
| |
· chlorination may be by direct addition of HTH or by diffusion from a porous pot chlorinator | |
| |
· continuous chlorination of point sources is expensive | |
| |
· it is preferable to identify and remove the source of contamination that to commit to long-term continuous chlorination | |
| |
· household chlorination may also be practised | |
| |
· this involves addition of solutions or tablets in the home |
|
|
|
· household chlorination is a short-term solution and rarely effective in the long-term | |
| |
· should never place an over-reliance on chlorination alone for treatment of water as can get outbreaks despite adequate disinfection, treatment and source protection are vital |
|
| |
· chlorination efficiency should never be compromised by concerns regarding risks from by-products | |
Disinfectants Evaluated
· Chlorine
· Chloramine
· Chlorine dioxide
· Ozone
· Iodine
Distribution of Hypochlorous Acid
and Hypochlorite Ion in Water at Different pH Values and Temperatures
Relationship between Measured Free
Residual Available Chlorine (HOCl+, OCl-) and
Bactericidally Active (HOCl)
Chlorine Demand
1. Make 1% chlorine solution2. Add 6 drops of solution to 1 litre of clean water
3. Mix well & leave for 30 minutes
4. Free residual should be 1.5-2.0 mg/l, if not either add more drops or dilute with clean water until this range is reached (this is original chlorine)
5. Measure out 500 ml into second container
6. Add 500 ml of water to be tested, mix well and leave for 30 minutes
7. Test water for free residual
8.

Breakpoint Chlorination
Source: Tebbutt, 1992
Types of Chlorine Commonly Available
· Calcium hypochlorite:
- powder containing 30-70% available chlorine
· Sodium hypochlorite
- solution containing 1-18% available chlorine
· Gaseous chlorine
- pure chlorine gas in cylinders
Chlorination in Piped Systems
· Chlorine is added post-treatment/post source· Maintain a residual at all points in network
· There should always be at least 0.2 mg/l free chlorine
· In time of cholera or other outbreak minimum is 0.5 mg/l in network and 1 mg/l at public standposts
· May get a reduction in residual during storage and distribution
· Therefore may need booster chlorination
Chlorination of Point Sources
· Chlorination usually only in times of outbreak· Use shock chlorination and maintain free residual of 1 mg/l
· Chlorine may be added by direct addition:
- HTH
- Tablets
· Chlorine may also be added through a porous pot diffuser· Can routinely chlorinate point sources if contamination always present but it is preferable to reduce contamination
· Point source chlorination may be difficult and expensive
Household Chlorination
· Only usually done in outbreaks· May be from tablet dosing or through solution
· Must be supported by health and hygiene education and risk reduction
· Household chlorination is expensive and rarely fully effective
· Household chlorination should be a short-term solution
Effectiveness of Disinfection
|
· 1966 - New Delhi |
Hepatitis outbreak despite adequate chlorination |
|
· 1966 - Scotland |
40-50% Dysentery S. sonnei/viral. Due to switch failure |
|
· 1961-1970 |
26,546 cases of GI due to contaminated water supply in U.S.A. |
|
· 1971-1972 |
5,615 outbreaks of GI due to Rotavirus and Parvovirus in small water supplies |
|
· Paris |
Poliovirus detected in water supply despite adequate treatment |
|
· U.K. |
20% of water sources in Wales have virus contamination |
Risks and Benefits of Water
Chlorination
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Water Treatment Chemicals and Construction Materials
Session Objectives
· To describe the sources of contamination deriving from water treatment chemicals and construction materials.· To demonstrate the need for product control rather than water quality analysis in controlling contamination from these sources.
· To describe some key contaminants deriving from the use of polyelectrolytes, PAHs and PVC.
Introduction
Chemical contaminants in drinking-water may originate from a variety of sources, including treatment chemicals used in the production of drinking-water or from materials of construction which come into contact with water during treatment, storage and distribution.
A listing of some chemicals used in water treatment, and drinking-water system components such as pipes, joining and sealing materials, process media and mechanical devices is given in Annex 1. Both chemicals and system components may release contaminants into the drinking-water (1, 2).
Processes used for manufacturing of water treatment chemicals may result in the presence of impurities that are of potential health concern. For example, a wide range of polyelectrolyte are used as coagulant aids in water treatment, and the presence of residues of the unreacted monomer may cause concern. Many polyelectrolytes are based on acrylamide polymers and copolymers, in both of which the acrylamide monomer is present as a trace impurity. Some polyelectrolytes may release epichlorohydrin, formaldehyde, ethylene dichloride or ammonia into the water. Chlorine used for disinfection has sometimes been found to contain carbon tetrachloride and mercury. Metals such as As, Ba, Cd, Cr, Pb, Hg, Sn, Se, and Ag may be found as impurities in a variety of water treatment chemicals.
Contaminants may originate from construction materials: metals such as copper, lead and cadmium are released from pipe material and solder; asbestos fibres from the inner walls of asbestos-cement pipes; polynuclear aromatic hydrocarbons from coal-tar-based pipe linings and coatings on storage tanks; traces of unreacted vinyl chloride monomer from PVC pipes; organic chemicals from in situ polymerized and solvent-applied coating; and radionuclides from sand and granular activated carbon used as filtration media.
Ensuring the safety of water treatment chemicals and construction materials
During the development of the 1993 WHO Guidelines for Drinking-water Quality, the subject of potentially hazardous chemicals in drinking-water derived directly from treatment chemicals or construction materials used in water supply systems was discussed. The conclusion reached by the experts was that such chemicals are best controlled by the application of national regulations governing the quality of the products themselves rather than the quality of the water.
For this reason, the Guidelines have not specifically addressed contaminants derived from water treatment chemicals, construction materials, paints or coatings. Nevertheless some of the contaminants arising from these sources were evaluated because of their world-wide importance and include, for example, asbestos, vinyl chloride, acrylamide, epichlorohydrin, di(2-ethylhexyl) adipate and phthalate, and benzo[a]pyrene.
National authorities in some countries such as the Netherlands (3), the United Kingdom (4) and the United States of America (2) have issued specification and recommendations for chemicals and construction materials thus ensuring the safety of the water delivered to the consumer.
Where specifications have not been developed, contamination from these sources may adversely affect the quality of drinking-water.
National drinking-water standards (or WHO guideline values, GVs) may be used to derive limits for impurities in water treatment chemicals. Using the approach adopted by the US National Research Council and National Sanitation Foundation (NSF) (2, 5), a recommended maximum impurity content (RMIC) in the treatment chemical is calculated using the following equation:
were NS is the national standard (or GV), and MD the maximum dosage of the water treatment chemical. A safety factor (SF) of 10 is judged as reasonable to limit to 10% of a given NS the contribution by a given impurity in a water treatment chemical. A sample calculation of a RMIC is as follows:
Contaminant (Pb): NS = 0.02 mg/litre
Water treatment chemical: Maximum dose (MD) 500
mg/litre
Safety Factor 10

If a national drinking-water standard (or WHO GV) is not available, new toxicity testing and evaluation may be necessary.
The concentration of contaminants released from products used in contact with drinking-water may be initially high, but rapidly decline with continued product contact with water. The NSF has adopted an approach whereby leachate tests are conducted to determine the slope of the contaminant concentration curve. If the initial (day 1) laboratory concentration of the contaminant is less than or equal to the 90-day No-observed-adverse-effect level (NOAEL), divided by 100, and the contaminant concentration is calculated to be at or below 10% of the national standard, then no additional toxicity data may be required.
Polyelectrolytes used in water treatment
A wide range of polyelectrolytes are available and the presence of unreacted monomer may cause concern. For example acrylamide polymers and epichlorohydrin-based polymers may release in drinking-water the unreacted monomers acrylamide and epichlorohydrin. To control this type of contamination, some countries have established maximum authorised dose of polyacrylamide used as a coagulant in drinking-water treatment (range 0.25-1 mg/litre), and specified maximum acrylamide content in polyacrylamide (varying from 0.025 to 0.1%). A standard of 0.1% of monomer at a maximum dose of polyacrylamide of 0.5 mg/litre would correspond to a maximum theoretical concentration of acrylamide in water of 0.5 mg/litre (same as WHO GV of 0.5 mg/litre for an excess lifetime cancer risk of 10-5).
Because of concern about certain contaminants, Switzerland and Japan do not permit the use of polyelectrolytes, including polyacrylamide, in drinking-water treatment (6). Other countries, such as the United Kingdom, Germany and the USA, establish limits on contaminant levels and application doses, as described above, which they can monitor and enforce.
A WHO Consultant Group examined the health aspects relating to the use of polyelectrolytes in water treatment and recommended that:
(a) polyelectrolytes should be used only after careful evaluation of the toxic hazards of particular products(b) countries wishing to use polyelectrolytes should establish a national committee to evaluate potential health hazards arising from their use
(c) limits should be specified both for the maximum applied dose of a polyelectrolyte and for its content of toxic monomer.
Polynuclear aromatic hydrocarbons (PAHs)
PAHs are present in the environment from both natural and anthropogenic sources. A GV of 0.7 pg/litre corresponding to an excess cancer risk of 10-5 was recommended for benzo[a]pyrene. There were insufficient data available to derive GVs for other PAHS. The following recommendation was made in the Guidelines for the PAH group:
"Contamination of water with PAHs should not occur during water treatment or distribution. Therefore, the use of coal-tar-based and similar materials for pipe linings and coatings on storage tanks should be discontinued. It is recognised that it may be impracticable to remove coal-tar linings from existing pipes. However, research into methods of minimising the leaching of PAHs from such lining material should be carried out"
Asbestos-cement pipes
Because of the lack of evidence for any health risk from ingested asbestos, no GV was proposed in the Guidelines for asbestos in drinking-water (see WHO Press Release attached in session V). However, one concern with A/C pipes is that cement is subject to deterioration on prolonged exposure to aggressive water - due either to the dissolution of lime and other soluble compounds or to chemical attack by aggressive ions such as chloride or sulphate - and this may result in structural failure of the A/C pipe. The American Water Works Association has set specifications for the type of A/C pipes to be used for different degree of aggressiveness of the water, as reflected in the "aggressiveness" Index or the Langelier Index. Pipes made of A/C, as well as almost all other materials, may not perform satisfactorily when in contact with highly aggressive water. Adjustment of certain water quality parameters, such as pH, alkalinity and/or hardness, may thus be necessary to control cement corrosion.
PVC pipes
Contaminants that may leach from PVC material include di(2-ethylhexyl) phthalate used as a plasticizer, antioxidants such as phenols and aromatic amines, lead, cadmium and organotin compounds used as heat stabilizers, acrylic processing aids, and residual vinyl chloride monomer (VCM). Based on cancer risk assessment, a GV of 5 µg/litre has been recommended for VCM by WHO, corresponding to an excess cancer risk of 10-5.
Low concentrations of VCM have been detected in drinking-water as a result of leaching from PVC pipes used in water distribution systems. A number of product standards exist which specify a quality of PVC pipes that limits the quantity of free VCM present. For example, NSF-International requires that the residual vinyl chloride monomer content of PVC material as determined in the wall of the finished product should be less than or equal to 3.2 mg/kg (2).
The European Union has set a maximum VCM level of 1 mg/kg in materials made of PVC which are intended to come into contact with food (or drinking-water). It is further specified that VCM should not be detected in food (or drinking-water) at the limit of detection of 0.01 mg/kg (7). In order to enforce these standards, the European Union has specified the methods of analysis of VCM in PVC material (8), and in food or water (9).
The use of PVC pipes has been reviewed by a WHO Consultant Group, with special emphasis on leaching of heavy metal stabilizers and associated impurities from the pipe wall. Additives such as lead, organotin and cadmium may be used in PVC pipe production. Other potentially hazardous compounds such as mercury may occur as impurities in PVC pipe. The Group recommended that:
(a) National standards for PVC pipes should be developed setting limits on the amount of toxic stabilizers that can be extracted from the pipe.(b) The International Organization for Standardization (ISO) should be regarded as the appropriate international body for the co-ordination of national standards and the development of uniform test procedures related to the extractability of toxic substances from PVC pipes.
(c) The use of cadmium compounds in PVC drinking-water pipe formulations is considered to be highly undesirable.
(d) Research should be carried out to determine leaching pattern of organotin stabilizers. Toxicological data on these materials are also needed in order to establish a tolerable daily intake.
(e) Toxic ingredients should be limited to the absolute minimum required for pipe production.
ISO has specified a test method for the determination of the extractability of prescribed constituents from the internal surface of plastic pipes, including PVC pipes, for the transport of water intended for human consumption. The constituents considered include monomers, initiators, emulsifiers, stabilizers, antioxidants, lubricants, polymers and copolymers for blends, UV absorbers, fillers and pigments. The method is applicable to extractable contaminants such as VCM, lead, tin, cadmium and mercury occurring as impurities in PVC materials. The purpose of the method is to verify that the extracted quantities do not exceed specified limits. However, ISO does not establish permissible limits for the quantities extracted (10).
Conclusions
Contamination of drinking-water by water treatment chemicals and construction materials may be controlled by the application of national specifications and regulations on the quality of the product. To support countries in developing control procedures for water treatment chemicals and construction materials, the Working Group on Protection and Control of Water Quality of the Rolling Revision of the Guidelines will prepare a monograph on the techniques for testing and control of materials and chemicals, ready for publication in 2001. This will be co-ordinated by NSF International in conjunction with the International Programme on Chemical Safety (IPCS).
In addition to the evaluation of chemicals as contained in the WHO Guidelines for Drinking-Water Quality, the IPCS has, in its Environmental Health Criteria documents, assessed the risk of several chemicals of direct relevance to water treatment and distribution systems: phenol, chlorophenols, mercury, lead, cadmium, tin and organotin compounds, tributyltin compounds, arsenic, Polycyclic aromatic hydrocarcarbons, aluminium, etc. International risk assessment from exposure to these chemicals will assist national authorities in identifying problem areas and in establishing specifications for chemicals and materials which come into contact with drinking-water.
References
1. American Water Works Association (1990) Water quality and treatment. 4th ed. McGraw-Hill. New York.
2. National Sanitation Foundation. Standard ANSI/NSF 60-1988 Drinking-water treatment chemicals-Health effects; Standard NSF 61-1991 Drinking-water system components-Health effects. NSF International. Avenue Grand Champ 148. 1150 Brussels, Belgium. Tel. 322-7713654; Fax 322-763-0013.
3. KIWA Ltd. Procedure to obtain a certificate of no objection on toxicological grounds. Rijswick, the Netherlands.
4. United Kingdom Committee on Chemicals and Materials. List of substances, products and processes approved under regulations 25 and 26 for use in connection with the supply of water for drinking, washing, cooking or food production purposes (December 1994). Drinking-water Inspectorate, Room B153, 43 Marsham Street, London SWIP 3PY. Facsimile: 44-71-2768405; Telephone 44-71-276-8901.
5. US National Research Council (1982) Water chemicals codex. National Academy Press, Washington, D.C.
6. Letterman, R.D. and Pero, R.W. (1990) Contaminants in polyelectrolytes used in water treatment. J. Am. water works Assoc. Vol 82, pp. 87-97.
7. Council of the European Communities Directive of 30 January 1978 on the approximation of the laws of the Member States relating to materials and articles which contain vinyl chloride monomer and are intended to come into contact with foodstuffs (78/142/EEC).
8. Commission of the European Communities Directive of 8 July 1980 laying down the Community method of analysis for the official control of the vinyl chloride monomer level in materials and articles which are intended to come into contact with foodstuffs (80/766/EEC)
9. Commission of the European Communities Directive of 29 April 1981 laying down the Community method of analysis for the official control of vinyl chloride released by materials and articles into foodstuffs (81/432/EEC).
10. ISO (1990) International Standard 8795 Plastics pipes for the transport of water intended for human consumption - Extractability of constituents - test method. ISO, P.O.Box 56, 1211 Geneva 20, Switzerland.
ANNEX 1
I. DRINKING-WATER TREATMENT CHEMICALS
Coagulation and flocculation: acrylamide copolymers, aluminium chloride, aluminium sulphate, bentonite/montmorillonite, cationic polyacrylamide, diallyldimethyl ammonium/chloride acrylamide copolymer, ferric chloride, ferric and ferrous sulphate, kaolinite, poly (diallyldimethyl ammonium chloride), polyaluminium chloride, polyamines, starch, polyethyleneamines, resin amines, sodium aluminate.
pH adjustment: calcium carbonate, calcium hydroxide, calcium oxide, carbon dioxide, magnesium oxide, potassium hydroxide, sodium bicarbonate, sodium bisulfate, sodium carbonate, sodium hydroxide, sulfuric acid.
Corrosion control: dipotassium orthophosphate, disodium orthophosphate, monopotassium orthophosphate, phosphoric acid, polyphosphoric acid, potassium tripolyphosphate, sodium calcium magnesium polyphosphate, sodium polyphosphate, sodium zinc polyphosphate, tetrasodium pyrophosphate, zinc orthophosphate.
Corrosion inhibitor: sodium silicate
Sequestering: ethylenediamine tetraacetic acid (EDTA), tetrasodium EDTA
Disinfection and oxidation products: anhydrous ammonia, ammonium hydroxide, calcium hypochlorite, chlorine, iodine, potassium permanganate, sodium chlorate, sodium chlorite, sodium hypochlorite.
Fluoridation: ammonium hexafluoro silicate, calcium fluoride, fluosilicic acid, magnesium silico fluoride, potassium fluoride, sodium fluoride, sodium silico fluoride.
Defluoridation: aluminium oxide, bone charcoal, tricalcium phosphate, high-magnesium lime. Algicide: copper sulphate, copper triethanolamine complexes. Softening: calcium hydroxide, calcium oxide, sodium carbonate, sodium chloride.
Taste and odour control: activated carbon, chlorine, chlorine dioxide, copper sulphate, ozone, potassium permanganate.
Dechlorinator and antioxidant: sodium metabisulfite, sodium sulfite, sulfur dioxide.
II. DRINKING-WATER SYSTEM COMPONENTS
Pipes and related products: copper, lead, stainless steel, brass, galvanized, concrete pressure, ductile iron, PVC, chlorinated PVC, asbestos/cement.
Protective (barrier): materials: coatings, paints, linings.
Process media:
Adsorption media: activated alumina, granular activated carbon, powdered activated carbon.Filtration media: aluminium silicates (e.g. zeolites), anthracite, diatomaceous earth, gravel, sand, membranes.
Ion exchange: ion exchange resins.
Mechanical devices: chemical feeders, pressure gas injection systems, disinfection generators, electrical wire, pumps, valves and related fittings, water process treatment devices (e.g. mixers, reverse osmosis, screens, clarifiers, aeration equipment, etc.).
Presentation Plan
|
Section |
Key points |
OHP |
|
Introduction |
· chemical contaminants in drinking-water originate from a variety of sources. | |
| |
· these sources include the water treatment process itself through the presence of impurities in the water treatment chemicals, drinking-water system components and contaminants originating from construction materials | |
| |
· some of these, such as polyelectrolytes, PAHs, copper, lead and cadmium are of potential health concern | |
|
Ensuring the safety of water treatment chemicals and construction materials |
· national regulations governing the quality of the products (i.e. the construction materials and treatment chemicals rather than the quality of the water itself is used to control potentially hazardous chemicals in drinking-water) | |
| |
· national drinking-water standards (or WHO Guidelines) may be used in a standard formula to derive limits for impurities in water treatment chemicals. Where national drinking-water standards are not available new toxicity and evaluation may be required |
|
| |
· the concentration of contaminants released from products used in contact with drinking-water may decline with continued product contact with water. Leachate tests determine the slope of the contamination concentration curve |
1 |
|
Poly-electrolytes used in water treatment |
· polyelectrolytes are widely available and the presence of unreacted monomers may cause concern. These may be released by certain polymers in drinking-water | |
| |
· as a result of the concern some countries do not permit the use of polyelectolytes in drinking-water or establish limits on contaminant levels and application doses | |
| |
· the health aspects relating to the use of polyelectrolytes in water treatment have been identified by a WHO Consultant Group and recommendations made for their use | |
|
Coalton linings |
· may release PAHs |
3 |
| |
· these are present in the environment from both natural and anthropogenic sources | |
| |
· a GV for benzo[a]pyrene has been established | |
| |
· it has been recommended in the Guidelines that where materials from which PAHs may leach are used, for example in pipe linings and coatings on storage tanks, alternative materials are used | |
| |
· Guidelines recommend alternative materials where PAHs may leach | |
|
Asbestos-cement pipes |
· there is no GV for asbestos in drinking-water as there is no evidence that asbestos has any adverse effect on human health when ingested with drinking-water |
4 |
| |
· concern that cement in asbestos-cement pipes may deteriorate after prolonged exposure to 'aggressive' water | |
| |
· specifications have been set for the types of pipes used depending on the degree of 'aggressiveness' - using the'aggressiveness' Index or Langelier Index | |
|
PVC pipes |
· a variety of contaminants may leach from PVC pipes. |
5 |
| |
· a GV has been set by the WHO for one of these - residual vinyl chloride monomer (VCM) - of 5 mg/litre based on a cancer risk assessment |
|
|
|
· low concentrations of VCM have been detected in drinking-water due to leaching from PVC pipes. The use of PVC pipes has been reviewed by a WHO Consultant Group and recommendations made for their production and use | |
| |
· the EU has set standards for the amount of VCM in materials made of PVC which are intended to come into contact with food or drinking-water. |
|
|
|
· a standard test method has been specified for the determination of the extractability of prescribed constituents from the internal surface of plastic pipes used for the transport of water intended for human consumption | |
|
Conclusions |
· control of contaminants from materials and chemicals used in treatment and distribution of water are best control through product control, not water quality monitoring | |
| |
· control of contamination of drinking-water by water treatment chemicals and construction materials may be addressed by national standards and regulations on the quality of the product | |
| |
· WHO is actively pursuing status to provide information on approved products and quality standards to Member States | |
| |
· the risk of several chemicals of direct relevance to water treatment and distribution systems has been assessed | |
| |
· international risk assessment from exposure to these chemicals can assist national authorities in identifying problem areas and establishing specifications for chemicals and materials in contact with drinking-water. |
|
NB: Annex 1 may be given as a handout as this is not included in the Guidelines.
Calculating Recommended Maximum Impurity Concentration (RMIC)
e.g. Pb NS = 0.02 mg/l; MD = 500 mg/l; SF = 10

Recommendations of the WHO Consultant Group on Polyelectrolytes
· Polyelectrolyte should be used only after careful evaluation of the toxic hazards of a particular substance.· Countries wishing to usepolyelectrolyteshould establish a national committee to evaluate potential health hazards arising from its use
· Limits should be specified both for the maximum applied dose of apolyelectrolyteand for its content of toxic monomer
Coalton Linings
· May release PAHs.· These are present in the environment from both natural and anthropogenic sources.
· Guideline value for benzo[a]pyrene has been established.
· Guidelines recommend alternative materials should be used where PAHs may leach.
Asbestos-cement Pipes
· No guideline value for asbestos.· May deteriorate after prolonged exposure to 'aggressive' water.
· Specifications have been set using the 'aggressiveness' Index/Langelier Index.
PVC Pipes
· A variety of contaminants may leach form PVC pipes.· Guideline value has been set for residual vinyl chloride monomer (VCM).
· Low concentrations of VCM have been detected in drinking-water due to leaching from PVC pipes.
· Standard test methods developed for 'extractability' of prescribed constituents.
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Institutional Frameworks
Session Objectives
· To describe the key players in the water sector and describe their roles and interaction.· To describe how the water supply sector should be structured and emphasise the need for a clear institutional framework to be established.
· To demonstrate the need for inter-sectoral and inter-institutional collaboration at all levels.
· To describe the key elements of legislation required for effective monitoring linked to water supply improvement.
Introduction
As the purpose of water supply surveillance is to promote the improvement of water supply services, it is important that the organisational arrangements intended to facilitate this pay due consideration to the vital and complementary roles of both the surveillance and the supply functions. It is also essential when establishing or reviewing the institutional arrangements of the sector with respect to surveillance and monitoring functions, that the most appropriate institution takes responsibility for surveillance functions.
Selecting Institutions and Assigning Responsibilities
There are a numbers of issues in deciding institutional homes for different functions and when doing this, it is important that the purpose of each function is clearly defined and matched against the overall remit of the institution. The principal functions concerned are: surveillance; supply, and; resource management.
Surveillance - Ministry of Health
It is preferable that because quality surveillance is concerned with human health, responsibility is assigned to the Ministry of Health as the agency responsible for the protection of public and environmental health. This is an independent monitoring role which takes into account water quality up to the point of consumption and for all the population, regardless of the source of water. This is clearly separate from quality control monitoring of water production and supply exercised by water suppliers within their area of supply. The separation of surveillance and supply functions is desirable to prevent any actual or perceived conflicts of interest from occurring.
However, given changing political structures and responsibilities for water supply, it may often not be practical to make the Ministry of Health responsible for field data collection as they may lack the necessary staff, skills and resources. The Ministry should, however, always maintain a national profile in water quality surveillance as a key preventative health activity.
Operational surveillance activities may be undertaken by local government environmental health bodies, with the Ministry of Health playing a co-ordinating and facilitating role. In many ways, this is the preferred scenario if local government does not have responsibility for water supply. Where local government also assumes responsibility for water supply, there may potentially be a conflict of interest. In such circumstances they may be financial and political objections to a centralised system of surveillance operated by the Ministry of Health. In these circumstances, there must be clear separation of responsibility for supply and surveillance up to the most senior levels, or an alternative body established taking responsibility either for supply (which is usually the favoured course) or surveillance.
Where a government department takes overall responsibility for development of water supplies, there may be some scope for them to undertake routine monitoring if the supplies are operated by another entity, although clearly it is questionable if they can be truly independent. Alternative bodies to the Ministry of Health can take responsibility for surveillance - for instance the environment sector - but as these are not health bodies, the Ministry of Health must retain a strong interest in the operation of surveillance networks and the data produced.
Quality control - Water supply agency
The water supply usually has a responsibility to ensure that the water supplied up to the connection with a house main or connection with a standpost riser or point of exit from a point water supply is of a wholesome nature and is fit for consumption. Usually this is measured against national standards and norms of water supply. This is separate function to surveillance as it is not concerned with the quality of water as consumed but of the water as supplied.
The meeting of national standards is usually a legal requirement which is enforced through surveillance. The frequency of quality control sampling, the techniques used and methods of quality control and reporting are generally standardise where piped water supplies operated by a supply agency serve a population of consumers. Where community based water supplies are used, whether point or piped, the supplier cannot usually reasonably be to undertake routine quality control monitoring and under these circumstances it is common that either only surveillance activities are undertaken or that the agency responsible for the development of community supplies to carry out quality control monitoring in addition to the surveillance function undertaken by environmental health staff.
Water resources - Resource management agency
A further complication to the institutional arrangements is when an independent water resource management/natural water quality monitoring body is established. This is an appropriate system where sufficient resources exist to fund the functioning of two regulatory bodies. The roles and responsibilities of natural and drinking-water regulatory bodies are very different and different types of qualification and experience are desirable in each. However, where resources are limited, it is sometimes found that the same body takes responsibility for both natural and drinking-water quality. This is not an unreasonable approach to be adopted, provided that a balance can be struck between the needs of both can be maintained. This is not necessarily easy, particularly where financial resources are scarce and has proven to be difficult to operate in many countries, usually to the detriment to drinking-water quality surveillance and protection.
When both forms of monitoring are placed within the same organisation there can be conflicts in approach and priority. For instance, the drinking-water quality surveillance arm, whilst recognising the need for protection of water quality in sources used for drinking, may not be sympathetic for the need to maintain water quality in water bodies exploited for other uses such as industry. Additionally, the drinking-water surveillance arm will place a higher priority on the quality of water in the supply system (i.e. during treatment and afterwards) than on raw water quality. On the other hand of course, the natural water quality monitoring arm will place great emphasis on the need to protect natural water quality and may attach little importance to post-treatment contamination on small scales. There is also a problem in that drinking-water quality standards are inherently stricter than most environmental standards and require a greater frequency of analysis. Again this may lead to difficulties in prioritising investment of limited resources.
Sector Structures
There are a number of different ways the sector can be structured and it is preferable to simplify this rather than create too many institutions with similar responsibilities. This not only makes enforcement difficult, it is confusing to the public who become unsure as to whom they should approach for action in the event of a problem.
Despite the many different institutional models that are available world-wide, the mostly commonly applied (and probably most simple model) is one where there are three principal institutions:
1. Water supply and sanitation agency(s);
2. Drinking-water supply surveillance body;
3. Water resource management agency - this may include pollution monitoring inspectorates.
The relationships between surveillance body, supplier and water resource management body should be clearly defined from the outset and in particular the legal framework within which they operate should be simple, clear and effective. What is of greatest importance is to define the limit of responsibility of each of the two regulatory bodies.
In general, the water supply surveillance body takes responsibility for the water once it enters the water supply system (the intake) up to the point of consumption (the tap). The water resource management agency takes responsibility for the development, management and protection of natural water and therefore their responsibility is for source waters up to the point of abstraction for use and from the point of discharge of return flows of wastewater. The water supply agency is obviously responsible for the integrity of it's infrastructure and effectiveness of any source protection or treatment applied to the water. There responsibility is therefore to produce a product of acceptable quality and have a responsibility from the point of abstraction to the point of connection with a house main or standpost riser or to the point of collection in point water supplies. This situation is complicated where the vending of water supplies at communal water points is licensed to water vendors, as they also have a responsibility to maintain the integrity of the riser pipe and fittings on the standpost and for timely reporting of faults to the bulk supplier.
Surveillance agency
The surveillance agency should preferably be established by national legislation and have representation at policy-making and all executive levels (such as central, departmental, regional, local or district levels).
The responsibilities of the surveillance agency should encompass monitoring of the fulfilment of water supply service standards by the water suppliers, approval of drinking-water sources (subject to specific treatment requirements where appropriate); and surveying the provision of drinking-water to the population as a whole.
Surveillance is concerned with all types of water used for domestic purposes by the population as a whole. This is a fundamental distinction to the role of the supplier who should be responsible only for the quality of the service they provide in the area in which they operate. The area of responsibility of the surveillance agency should ideally encompass all sources of water intended for human consumption. In practice this is often difficult to achieve as many households or small communities may have individual supplies (whether a single household well or spring or a small piped distribution system). As the number of such systems may be very high, the surveillance of all such supplies may be a costly and difficult-to-achieve goal. Priority should therefore be given to:
· systems supplying water to larger centres of population;· systems suspected of being a risk to human health; and
· to be a representative sample of other types of supply in order to identify the most common shortcomings of these.
Water supplier
The above does not exclude water supply and construction agencies from involvement in surveillance and in fact it is vital that they are involved.
While it is the responsibility of the surveillance agency to generate and summarise surveillance data and to promote improvements, it is the supply agency who will carry out many of the actions for improvement.
Supply agencies also have an obligation to monitor and control the quality of the product they supply, in common with the suppliers of any other types of product. This function is often referred to as quality control in order to distinguish it from the health-related surveillance function performed by the surveillance body.
In many countries arrangements to share water quality data exist between surveillance and supply agencies. In some these arrangements are informal and instigated at local level. In other cases they are formalised and the surveillance agency accepts data generated by the supplier in place of some of the data it would otherwise generate itself, provided the laboratories of the supply agency are open to inspection and the surveillance agency maintains a realistic minimum proportion of analyses for overseeing purposes.
Water resource management agency
The water resource management agency monitors natural water quality and wastewater discharges. They will also licence abstraction, monitor industrial discharges etc., but their key role within water supply is to protect source water quality so that it remains at a quality consistent with use in drinking-water supplies and for ensuring that return flows do not cause deterioration in natural water quality. They should have the power to prosecute water and sewerage agencies for failure to meet wastewater quality standards and to monitor water abstractions to ensure compliance with agreed limits.
The water resource management agency may also monitor natural water quality changes due to leakage from water supply pipes and sewers and have the power to force suppliers to carry out remedial action to improve performance in order to protect natural water quality. This is particularly important in relation to groundwaters in urban areas, where excessive leakage from sewers or water supply pipes will affect natural groundwater quality.
To a certain extent this overlaps with responsibilities undertaken by the water supply surveillance agency as they too will monitor leakage, albeit from a health related stance. This provides a good illustration of the need for strong inter-institutional links and for clear definition of responsibility. In principle, both the water resource management and the surveillance body could take enforcement action against the water and sewerage supplier, or bring a joint action. In practice, this frequently does not occur as, for instance, the surveillance body may not be interested in pursuing an action where they see no direct harm to the water supply.
Inter-Agency Collaboration
What is clear from the above is that there needs to be strong inter-agency collaboration if the water sector is to function effectively and efficiently (See Figure 1). There are many potentially overlapping roles and conflicting interests. Many of the problems that arise within the water sector are caused by a lack of dialogue and a certain element of shirking responsibility which can only be resolved through adequate dialogue.
To provide an example, imagine a situation where the water resource management agency grants a discharge consent to a chemical company several kilometres upstream from a water supply intake. The plant is discharging halogenated organic material. Neither the water supply agency or the surveillance body are consulted and the plant starts to discharge. Some while later, the surveillance body starts to detect raised levels of halogenated organics in the water supply and therefore initiates action against the water supplier.
The water supplier, by identifying the elevated level of pollutants in the source water could ask the water resource management agency to prosecute the polluter in order to cover the costs of installing expensive additional treatment processes. As the polluter has a discharge consent and meeting the conditions of that consent they can argue that they are not liable for this. This leads to a situation where no-one will take responsibility for improving the quality of the water supplied to the consumers. In this situation the water supplier and surveillance agency could make a case against the water resource management body for negligence of duty.
The scenario outlined above may seem unlikely, but similar incidents have occurred worldwide. If a process of dialogue is maintained between all parties at all levels, these incidents should not occur as there will be thorough evaluation of impacts from all points of view. Taking the example above, the water resource management body would be expected to undertake an environmental impact assessment of the discharge. However, this may or may not include influences on the water supply itself and may not look at human health impacts of ingestion of contaminated water. If a combined assessment had been undertaken, including looking at treatment implications for the water supplier and the health impacts, a more clearly defined picture could be built up about the discharge. This would be likely to change the terms of the consent and the cost of the consent to the industry.
Figure 1: Institutional framework
for the water supply and sanitation sector. Howard G., 1996
Laws, Regulations and Standards
Effective water supply monitoring programmes require the support of appropriate legislation, regulations, standards and codes of practice. Important aspects which should be considered in supportive legislation include:
· functions, authority and responsibility of the water supply agency· functions, authority and responsibility of the surveillance agency
· functions, authority and responsibility of the water resource management agency
· codes of practice regarding the notification of changes in source water quality to both supply and surveillance agencies by the resource management agency
· codes of practice regarding the construction, organisation and maintenance of facilities by water suppliers
· codes of practice regarding the construction of domestic facilities
· water quality standards and provisions for their updating
· procedures for authorisation of sources as suitable for drinking-water supply
· minimum treatment requirements according to source water quality
· requirements of disinfection and minimum residual disinfectant concentrations to be maintained throughout distribution
· procedures for approval of sampling and analytical methods for use in water quality laboratories and analytical quality control requirements of such laboratories
· requirements of water suppliers to undertake a defined minimum sampling programme
· guidelines on procedures to follow, including notifying and providing advice to the public if contamination of drinking-water occurs
· provision of legal recourse to the public and surveillance agency to initiate legal action to ensure adequate water supply service quality
· definition of 'adequate water supply service quality' with regard to parameters such as 'continuity'
· code of practice to ensure that discharge consents in a catchment are only granted after full consultation with supply and surveillance bodies.
However, it is important to recognise the limitations in a purely legislatively driven approach to water quality monitoring as a means of improving poor water supplies in low-resource situations. The development of partnership approaches and the encouragement of all stakeholders in the sector playing an active role in monitoring water supplies and identifying improvements may be more effective where resources are limited.
Conclusion
The development and optimisation of the institutional framework in the water sector is essential for effective, output driven water quality monitoring. Unless the roles and responsibilities of each player are established and recognised, then the generation of monitoring data and information may not lead to the desired improvement in water supplies.
Water quality is a multi-agency issue which requires effective collaboration from all the key stakeholders. Whilst, legislation plays a role in achieving this, it is important to note that partnerships between regulators, suppliers and consumers may be more effective in promoting good water quality, particularly where resources are limited.
References
Bartram, J and Ballance, R. (1996) Water Quality Monitoring, Chapman and Hall, London.
Howard, G. (1996) Urbanisation, Sanitation and Environmental Health, Commonwealth Secretariat, London.
Presentation Plan
|
Section |
Key points |
OHP |
|
Introduction |
· Surveillance is intended to promote water supply improvements |
1 |
| |
· Institutional arrangements are therefore vital | |
| |
· Surveillance and supply functions are distinct but complementary | |
|
Selecting Institutions and Assigning Responsibilities |
· Match the requirements of each function to the remit of the institution |
2 |
| |
· Ministry of Health is preferred for surveillance as this is a health-related activity | |
| |
· Separation of supply and control functions is important to reduce the risk of conflicts of interest arising | |
| |
· There are risks in over-centralising surveillance through the Ministry of Health as this may replicate local capacities and increase costs | |
| |
· Surveillance often best delegated to environmental or public health departments in local authorities | |
| |
· Where Government takes responsibility for water supply, the same body may undertake surveillance, provided there is adequate separation between functions up to the most senior level | |
| |
· An alternative approach is for water suppliers to generate monitoring data that is routinely submitted to the surveillance body | |
| |
· A water resource management body may sometimes undertake surveillance | |
| |
· Advantage of this approach is that it minimises replication of equipment and facilities | |
| |
· However, the remit of surveillance and other activities must be clearly defined and surveillance given adequate priority | |
|
Sector Structures |
· These should be simple to optimise performance |
3,4 |
| |
· Most common model is based on 3 agencies: surveillance agency; water supplier; resource management agency | |
| |
· Clearly define relationships and legal framework from the outset |
|
|
|
· Suppliers responsibility is from intake to connection of supply main to house main and house connection to mains sewers to the point of effluent discharge | |
| |
· Surveillance agency responsibility runs from source to the point of consumption | |
| |
· Resource management responsibility is natural waters and wastewater discharges | |
| |
· Surveillance agency should be established by legislation and be represented at policy and all executive levels | |
| |
· Should monitor fulfilment of all water supply service standards |
|
|
|
· Should be a national body | |
| |
· When establishing surveillance programmes must prioritise activities | |
| |
· Resource management agency role is to monitor and control natural water quality and effluent quality |
|
| |
· Prosecutes polluters (including water and sewerage providers) when fail to meet standards | |
| |
· Monitor all impacts on water resources and take appropriate actions | |
|
Inter-agency collaboration |
· Inter-agency collaboration must be string for sector to function effectively and efficiently |
5 |
| |
· Dialogue reduces litigation and is more cost-effective | |
| |
· Give an examples of potential problems resulting from poor collaboration | |
|
Laws, Regulations and Standards |
· Laws, regulations and standards should cover all aspects of the water sector | |
| |
· Refer to legislative frameworks session | |
Institutional Framework
1. Surveillance and control monitoring are designed to promote improvement2. Institutional arrangements are vital
3. Responsibilities must be clear
4. Institutional responsibilities should be compatible with wider concerns
5. Surveillance, supply and resource management are complimentary
Key Sector Institutions
1. Water and sewerage service provider(s)2. Drinking water surveillance body
3. Water resource management agency - may include pollution inspectorates
Institutional Responsibilities
Surveillance agency:
· Monitor water supply quality to the population as a whole
· Authority to sample from anywhere in all water supplies
· Authority to enforce compliance
· Should establish a sanitary code
· Must keep the public informed
Supplier:
· Supply water meeting all national standards to consumers
· Exercise quality control and allow access to data
Resource Management Agency:
· Monitor natural water quality and pollution - enforce standards
· Protect and manage water resources
Limit of Institutional Responsibility
· Surveillance agency: Source to point of consumption
· Water suppliers: Source to house connection/point of collection
· Resource management agency: All water resources
Institutional Framework for the
Water
Sector
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Legislative Frameworks
Session Objectives
· To highlight the need for a clear and comprehensive legislative framework for the water sector as a means of promoting its effective functioning.· To describe the mechanisms for establishing legislation and outline the basic content of water sector legislation.
· To stress the need to view surveillance and quality control of water supply in a broader context and recognise the value of such programmes beyond simple compliance monitoring.
· To emphasise the risks of over-reliance on legalistic approaches to water quality and to promote greater openness regarding water quality information.
Introduction
A comprehensive and effective legislative framework is essential for the smooth operation of the water sector and for it to meet its goal of providing an adequate water supply. The key principle that should underlie the legislative structure of the drinking-water sector should be to protect and improve public health through the sustainable provision of drinking-water of adequate quality in sufficient quantities to all the population continually at a price which is affordable.
Water sector legislation is likely to be a collection of acts, codes of practice and regulations under a general water law which as a whole govern the functioning of the sector. It is unlikely that a single document would cover all aspects referred to within this paper and indeed this would not be advisable as it would make the legislation unwieldy and difficult to update. Legislation should be flexible and dynamic and respond to developments within the sector rapidly and coherently.
Within the legislative framework which governs the sector, some key areas must be addressed to provide the sector with the structure it requires to function efficiently and effectively. It is essential that the institutions undertaking different functions within the sector - supply, resource management and surveillance - are clearly identified. For each institution, the roles, responsibility and remit must clearly stated and the type and level of interaction between each body must apparent.
Legislation is a tool to incorporate water policy within the national political-legal framework and should aim to protect both individual and communal water rights issues. Water quality is therefore only one aspect of water legislation which should cover aspects such as quantity of water supplied, access assurances, continuity provisions and limits set on costs charged to consumers. The legislation will empower the surveillance bodies, both financial and health-based, to closely monitor the water supplier to ensure that they met statutory functions which guarantee the supply of wholesome drinking-water.
However, it is also important to keep legislation within perspective and not allow an overly-legalistic approach to be developed towards water quality and supply. For instance, it is clear that surveillance of drinking-water supply has a value independent of legislation or enforcement of compliance. As it should be an activity primarily designed to identify risks, the primary concern should be to influence management decision making to reduce risks to public health.
The lack of provision in the legislation or lack of will to prosecute water suppliers for noncompliance should never be used as a pretext for abandoning surveillance activities. Some authors have suggested that surveillance is pointless without the political will to enforce legislation. Such an approach fails to recognise the wider role of surveillance and the link to improved decision making. It is vital that legislation is seen as a tool which facilitates water supply improvement and not as an end in itself.
Establishing legislation
It is common to find that much of the water legislation in a country has historically been incorporated within other acts and elements of legislation, such as Public Health Acts or Natural Resources Acs. Whilst these may address water, it is limited to specific impacts and fails to provide a comprehensive framework for the sector. It is therefore desirable that all water legislation be brought under an umbrella Water Act which has an array of associated addenda, regulations and codes of practice.
A complicating factor in establishing water legislation will be the current level of water supply coverage and the plans for extending coverage of the total population with access to an adequate water supply. In particular, the legislative framework should take into account that a significant proportion of water supplies may be community managed and operated whilst others may rely on a water supply agency. Furthermore, in many countries there may be a mix of piped water supply with a high level (in-house) of service and communal point source or shared tap water supplies.
The standards which cover these different types of supply must be carefully considered - for instance to insist on the same standards of supply from a community-managed hand-dug well and a sophisticated treated and piped water supply based on tariff collection is unlikely to be feasible. Furthermore where the community is the water supplier, the implications for legislation are very different from situations where a revenue-generating agency operates a water supply.
It is therefore essential that national water legislation recognises the variation in water supply types and establishes a range of regulations and codes of practice which can be used as a flexible method of promoting water supply quality. In these circumstances, therefore, although the same legislation will cover all water supplies, the standards set for each type of supply will be different.
Key elements of legislation
Policy statement
The legislation must clearly outline the policy principles which underlie the development of comprehensive water laws which govern the sector and also gives clear indications to the long-term goal for the sector. Thus, the principle of equitable access to water sources and supplies for the whole population and establishment of guiding principles for the levels of service and quality of services provided should be outlined.
The policy statement should also clearly highlight source protection, minimum treatment requirements and water supply monitoring that is expected from the different institutions. The policy statement should also clearly state the different but complementary roles of the supplier and the surveillance agencies. It should be made clear that independent, health-based surveillance is essential and entails the routine monitoring of suppliers performance with respect to nationally and regionally accepted norms of practice.
The policy statement should also clearly state the underlying health related rationale for water supply in the country and the primacy of drinking-water supply in use of water resources. This should also clearly state the need for source protection and distribution maintenance as well as outlining the need for minimum treatment requirements for water supplies of all types.
Institutional roles
The different institutions, their remit and responsibility should be clearly defined within the legislative framework. Failure to provide this will lead to long-term problems within the sector from overlapping responsibilities, duplication of effort, unclear reporting lines and difficulties in enforcement.
By preference, the number of institutions active within the sector should be limited and not allowed to become overly complex. The actual responsibility of suppliers and surveillance agencies must be very precisely defined and the interaction between the two and the process of dialogue, direction and enforcement transparent. It is important that the need for an ongoing and effective inter-agency dialogue and co-operation is essential for the effective functioning of the sector. The legislation should provide the framework for dialogue and cooperation by establishing minimum acceptable procedures in terms of information sharing and action. However, the legislation should also try to encourage greater dialogue than merely the basic minimum.
For further information on the institutional framework of the sector, please refer to the session on Institutional Frameworks and to Volume 3 of the GDWQ.
Service levels
Service levels in this context are taken to mean the parameters such as quantity, continuity and accessibility of the water supply to the user community. These issues are as important was water quality aspects of water sector legislation and must be included within a policy statement or reference within the legislation.
Service levels will have to be addressed at several levels and may therefore be referenced at various points in the legislation. For instance, at a national level, service should be addressed through the statement of position regarding the basic right of all the inhabitants to have access a water supply of sufficient quality and quantity to meet all their needs. In the first instance this may only be included as the goal of the sector within the legislation, but it should act as the fundamental basis for water sector legislation.
Within the areas supplied by water supply companies, the minimum acceptable and optimal quantities of water to be supplies should be outlined as well as the continuity of supply and the coverage of supply. This is essential if suppliers are to be governed by a framework which allows to function effectively and efficiently.
Where water supplies are community managed, the legislation should provide a framework for the acceptable population using point water supplies or communal facilities and the maximum acceptable distances to water supplies allowable. The latter may not refer to the entire population of a community but, for instance, the 90 or 95 percentile in dispersed communities. This legislation is essential if NGOs and Government agencies are active within community water supply in the country.
Source protection, sanitary norms and minimum treatment requirements
The details of source protection measures expected at different types of water supply and dealing with immediate source surrounds and broader measures should be clearly outlined in standards and regulations. Thus information regarding sanitary completion of wells, boreholes and springs, land-use control within the immediate vicinity of the water source and within the broader recharge area should be included within the legislation governing water supplies.
The information should include the details of standard designs of point source water supplies and the acceptable sanitary norms to be enacted within the immediate vicinity of the source. This will include aspects such as the grouting of the upper levels boreholes, size and thickness of aprons and headwalls, pump fittings and fencing. For groundwater sources, the legislation should also reference the need the acceptable types of pumps (including make and model), acceptable pumping and lining materials in different conditions and training for operators in community based water supplies.
The need for broader protection measures of sources should also be covered and should include reference to groundwater protection policies and strategies at local and aquifer levels and the principles and broad categorisation of land-use zones surrounding groundwater and surface water sources given.
Minimum treatment requirements should be referenced and the requirements for different water sources clearly outlined. The importance of maintaining a free residual when chlorinating is practised should be emphasised. The need for maintenance of distribution systems should also be referenced, particularly with regard to maintaining chlorine residuals and the frequency and use of sanitary inspection outlined. Again, training requirements should be outlined.
Liability
The question of liability with respect to water supplies may arise from a variety of scenarios, including an outbreak of water-related illness, insufficient supply or discontinuity of supply. Liability will be an issue when an agency or company provide water to tariff paying consumers. In these circumstances, water supply is acting in part as an economic good and as such, a certain level of service and quality of service should be expected by the consumers. In these circumstances, failure to meet acceptable levels of service or failures in water quality leading to outbreaks of disease should make the water supplier liable for prosecution from either the surveillance agency or consumer groups.
However, whilst the above can be seen as being an fair position with regard to liability, caution must be exercised when pursuing a liability-based approach to enforcement of water supply standards. In all circumstances, the emphasis on liability will tend to make water suppliers both more defensive in accepting blame for water supply failure, thus possibly leading to a reluctance to undertake remedial work that is required as this may be interpreted as an admission of guilt. Furthermore, in the cases of an infectious disease outbreak, it may become more difficult to identify sources of contamination and routes of disease transmission as water suppliers become reluctant to cooperage fully with investigation teams. In many countries, where liability has been successfully pursued, a net result has actually been the reduction in availability of water supply quality data from suppliers who increasingly will only provide the minimum required.
Issues regarding liability should not arise when community water supplies are dealt with as in these circumstances, the consumers are also the operators and managers of the water supply. No attempt should be made in these circumstances to assign liability on a water supply basis. However, there may be a case of assigning liability to whichever Government agency responsible for extending water supply coverage within the country and where this agency fails to provide support to certain areas for non-justifiable reasons, appropriate action may be followed.
The surveillance agency also clearly has a responsibility to keep the users of water supplies informed about any deterioration in water quality or any events which may compromise health because of water supply problems. Failure to carry out these functions should make this agency liable, although again a common sense approach is required to judge whether failure to inform the public results from justifiable reasons (lack of resources, lack of available information etc.) rather than wilful dereliction of duty.
Liability is a difficult issues in the water sector and the degree to which the rules of liability apply will vary between countries. However, it must be recognised that whilst liability may be a final solution for achieving action to improve water supplies - whether from an individual supply agency or Government Department responsible for water supply coverage - it is rarely the most effective way of achieving improvements.
Monitoring and surveillance aspects
The legislative framework should clearly outline the responsibility for monitoring and assessment procedures and activities to be undertaken by suppliers and surveillance agencies. The regulations and standards which support legislation should cover the numbers of samples both agency should take routinely, the numbers of samples to be taken for non-routine assessments (for instance during source selection, periodic quality assessment of sources etc.) and the numbers of samples to be taken in the event of suspected failure in water quality.
The analytical range to be covered in routine monitoring, non-routine assessment and in outbreak investigations should also be outlined in the regulations. The definition of the parameters is best left out of the legal instrument itself but should be included as an addendum or similar document which can be easily updated on a regular basis. In addition, the regulations should also clearly reference standard analytical methods acceptable for different circumstances and also the sampling techniques etc. to be employed.
Where community-based water supplies are the norm, there will be no need to establish supplier monitoring requirements, but surveillance agency responsibilities should still be outlined. The legislation covering surveillance of community based supplies should be less demanding than supplier operated supplies unless sufficient resources will be made available to the surveillance agency to conduct routine monitoring activities on a regular basis.
Where community based supplies are widely used, these are likely to involve many small water supplies scattered over a wide geographical area. Thus to expect a similar level of surveillance activity as in piped supplier operated water supplies. Furthermore, this would be likely to divert resources required for funding improvements of water supplies or supporting community based development.
In community based supplies, the surveillance agency should have a requirement to promote and conduct sanitary inspection and critical parameter water quality analysis and have a clear remit to conduct water use and hygiene education. Legislation should emphasise the need for management-linked monitoring aimed at building capacity and not data collection for its own sake.
Reporting requirements and data access
The inter-institutional reporting of monitoring and assessment data and the public access to water supply quality information should also be clearly highlighted in the legislative framework of the sector. The requirements of suppliers to report water quality data both routinely and in the event of failure must be clearly stated. It must also be clearly stated to whom such reports must go to. The latter is particularly important in water quality failures as there may be other bodies (such as local health boards, national public health agency etc.) which require information in addition to the surveillance agency.
The feedback of information from the surveillance body to suppliers and communities is equally important and the requirements and procedures for doing this need to be at least referenced within the legislative framework, although the detail may be held within appropriate regulations.
Clear guidelines for reporting to the general public and general policies towards public access to water quality data should be outlined within the legislation. It is important that both surveillance agency and water suppliers function in a open and transparent manner which encourages public awareness. The general public, whether using supplier-operated or community-based water supplies, clearly have a right to water supply quality information in an comprehensible format. Thus, data should not presented in a form which is confusing to non-specialist readers as this will foster a belief that suppliers and surveillance agencies are hiding the true situation.
In addition to public access to water quality data, the legislation should outline or reference, issues regarding the access and use of raw data. In some countries, notably the USA, there is a strong belief in the right of access to raw data for the public to view and use. In many other countries, access to raw data is strictly controlled and very few people outside of the supply or surveillance agency can access or use such data and then only in certain ways set down in legislation. There are advantages and disadvantages to both approaches and the route followed is a national decision based, in part, on relevant national legislation on the freedom of information. It is, however, an important area to legislate for as a lack of a strong position may cause unnecessary confusion.
Water quality standards
Whilst it is usually preferable not to include the actual standards within the legal instrument, clear reference should be made to the process of establishing standards and make provision for regular updating of standards by the appropriate bodies. The approach of inclusion of standards within the legal instrument is often adopted as it is felt that this is the most effective way of ensuring that standards have a legal force. The problem with this approach is that it makes the process of standards revision time-consuming and unwieldy. This has implications for countries trying to progressively improve water quality through the use of interim standards and with respect to the increasing large and diverse range of pollutants found in drinking-water which are of health concern.
In less wealthy countries, where trying to achieve WHO Guideline levels of substances may not be feasible for some time and there is a need to progressively improve the water supply situation, an unwieldy legal framework may be counterproductive. As interim standards may be established which are progressively upgraded, the system for establishing these must be flexible. Equally, a rigid legal approach to standards may result in resources being used for inappropriate levels of compliance monitoring, rather than the use of monitoring to improve water supplies.
The increasing range and diversity of pollutants of health concern has implications for all countries, no matter what their level of socio-economic development. There are a great many substances, including many synthetic organics, which are now being found in drinking-water and whose impact on health is not conclusively proved. The acceptable limits for concentrations of these substances in water may change considerably as more information becomes available and therefore the legal instrument establishing these in the national legislation must be responsive to these likely changes.
A mechanism for overcoming these problems is to clearly refer to the process of standard setting, with the Minister responsible named and also clearly stated that this Minister will provide the national legislative body with the standards that their experts deem necessary for safeguarding the well-being of the population. Furthermore, it is important that standards are not set for substances for which no conclusive evidence exists of a risk to health. For these substances, guidelines are more appropriate and a research programme initiated to quantify the level of risk posed.
Interim standards and exemptions
Within the legislative framework, clear provision should be made for the establishment of interim standards where these will be adopted in the short or medium term. However, if interim standards are to be set, there must be clear rationale established for the need and desirability for interim standards and some indication given for the final standards being aimed for. It is unwise to reference standards as interim unless clear indication is given of the final standard as this will in all likelihood lead to inertia in updating standards and to pressure from suppliers to maintain sub-optimal standards, even when higher standards could be achieved.
An alternative to interim standards is the use of exemptions from meeting certain standards. These may be of particular value when the failure is restricted to certain geographical areas or affect a relatively small proportion of the population.
Within the legislation, the process for establishing exemptions should be clearly outlined and time limits set for the duration of an exemption. The whole purpose of exemptions is to allow for short-term deviations from proscribed water quality limits which are permitted whilst remedial work is carried out on a water supply or source with the aim to meet national standards. Therefore, when an exemption is issued, it should be clearly linked to a programme of work within a specified time which has clear aims and objectives. There is little point in issuing exemptions which are de facto permanent. In these cases it is more effective to establish either an interim national standard, establish a regional or supply type interim standard or establish tiered standards.
Exemptions should clearly relate to specific substances and should indicate the concentration of a particular substance which is being allowed and for what period. It should be clear that when an exemption is granted that this does not imply that the water quality is allowed to deteriorate beyond the stated limit of the exemption or for substances other than those indicated within the exemption. Thus, granting an exemption must not be interpreted as being a licence to provide poor quality water. It is merely a temporary relaxation of particular standards which is clearly linked to remedial action being carried out to meet the specified standard.
It is more effective to prepare a series of interim standards which are relevant to particular water supply types or geographical and which clearly link to a process of water supply improvement to meet microbiological standards within as short a time as is feasible.
The issuing of exemptions on microbiological grounds should be avoided for public health reasons and as this may establish a dangerous precedent on non-compliance with microbiological standards. If it is know that microbiological standards in some types of water supply or in particular geographical regions cannot be met, it is more sustainable to establish interim or tiered standards rather than an exemption. If, for instance, a standard to set which cannot be met in a small community piped water supply and these are provided with an exemption, this may be seen as a precedent for large supplier-operated water systems to also apply for an exemption.
Conclusion
The legislative framework of the water sector is a vital component in improving and maintaining water supply quality within a country. However, it is only one of several tools which facilitate this and the limitations of legalistic and liability-based approaches to water supply improvements must be recognised.
Legislation should be flexible and comprehensive in its coverage of the water sector and it should be easy to update standards governing the sector. Due consideration should be given to the nature of water supply within the country and the implications this has for legislative framework. However, it is essential that any water laws clearly identify the goals of the water sector and provide it with a framework within which these are achievable.
The institutional framework of the sector should be incorporated within the legislation and the roles, responsibilities, remit and accountability of each institution clearly outlined. Failure to this is likely to result in considerable overlap, duplication of effort and inefficient implementation of water policies.
Presentation Plan
|
Section |
Key points |
OHP |
|
Introduction |
· there is a great diversity of approaches to legislation world-wide |
|
|
|
· a comprehensive and effective legislative framework is essential for sector | |
| |
· legislation should be underpinned by the principle of protecting public health through the provision of drinking-water | |
| |
· legislation is likely include a basic water law supported by a collection of codes, regulations and standards which outline institutional responsibilities, remit of agencies, sampling frequencies, information sharing etc. | |
| |
· key aspects such as institutional responsibility and inter-institutional co-operation are key for the sector performance | |
| |
· legislation incorporates the water policy within the political-legal framework of the country and should guarantee communal and individual water rights | |
| |
· legislation should be kept in perspective and care must be taken not to develop an overly-legalistic approach to monitoring | |
| |
· surveillance has a value independent of compliance monitoring and is an important tool to promote water supply improvement | |
| |
· a lack of legislation or political will to enact legislation should not be used as a pretext for abandoning surveillance activities |
|
|
Establishing legislation |
· historical legislation often included in other legislation (e.g. public health act) | |
| |
· however, it is desirable to have an umbrella water act which governs the sector | |
| |
· establishing legislation may be complicated by community managed schemes and mixture of supply service level | |
| |
· standard and legislation covering different types of supply should be carefully considered and different conditions set for different types and levels of water supply | |
|
Key elements of legislation |
policy statement |
1 |
| |
· legislation must clearly outline policy principles underlying the development of water laws - this includes equitable access to water supply and service indicators | |
| |
· source protection, minimum treatment requirements and water supply monitoring should all be highlighted | |
| |
· the need and role of independent, health-based surveillance should be emphasised | |
| |
institutional roles | |
| |
· the institutions and their responsibilities and remit should be outlined in legislation | |
| |
· the number of institutions active in the sector should be minimised to prevent overlap and duplication of effort | |
| |
service levels |
2 |
| |
· includes: quantity, continuity and accessibility | |
| |
· these should be addressed at national, regional and local levels and the legislation should clearly outline the principle of the right of all the population to have access to an adequate water supply | |
| |
· water suppliers should be required to meet minimum levels of services | |
| |
· community-based approaches should highlight issues such as minimum acceptable distance to the supply and numbers of people per water point |
|
|
|
source protection, sanitary norms and minimum treatment requirements |
3,4 |
| |
· source protection requirements for all types of sources should be included in legislation | |
| |
· standard designs and acceptable sanitary norms around point sources should be clearly outlined in the legislation | |
| |
· the need for broader protection measures should also be covered, including protection zones and land-use control | |
| |
· minimum treatment requirements should be clearly outlined and the importance of maintaining disinfectant residuals emphasised | |
| |
liability |
|
|
|
· liability may result from a number of scenarios including disease outbreak, temporary interruption of supply or insufficient supply | |
| |
· where a water supplier levy water charges, they will become liable for failure to meet proscribed service levels | |
| |
· however, a liability approach alone will not necessarily lead to water supply improvement and may lead to a reduction in access to information |
|
|
|
· liability should not be ascribed for community managed water supplies | |
| |
monitoring and surveillance |
5 |
| |
· monitoring and surveillance procedures should be clearly outlined | |
| |
· these should include sampling frequency, numbers of samples, sample locations and analytical range for both supply and surveillance agencies |
|
|
|
· for community-based supplies no supplier requirements need be set, but surveillance agency requirements should be established | |
| |
· for community-based water supplies, greater emphasis should be placed on using monitoring to improve water supplies | |
| |
reporting requirements and data access | |
| |
· inter-institutional reporting and public access to water quality information are key aspects to be addressed by legislation | |
| |
· this should include routine monitoring data, reporting when failures occur and to whom reports should be sent | |
| |
· clear statement of principles concerning public access is required and where possible as much information as possible should be made available |
|
|
|
water quality standards |
6 |
| |
· don't include actual values of standards in legislation, but do clearly reference mechanism of establishing standards | |
| |
· including values in legal instrument makes updating of legislation difficult and makes legislation unwieldy | |
| |
· important for countries which adopt interim standards to be able to update these progressively | |
| |
· also important as many new pollutants recognised which must be covered by legislation | |
| |
· possibly use an addendum or a regulation to cover actual values of standards | |
| |
interim standards and exemptions |
7 |
| |
· where interim standards used, these should be covered in legislative framework, | |
| |
· make sure some reference is made to desired final standards |
|
|
|
· also may use exemptions where problems with meeting standards is restricted to defined geographical areas or particular technologies | |
| |
· exemptions should only be granted where a short-term deviation is to be permitted and should be allowed to become permanent | |
| |
· exemptions should relate to specific substances and clearly indicate the substance and the concentration covered by the exemption | |
| |
· exemptions should not be granted for microbiological quality - use interim standards instead | |
|
Conclusion |
· legislative framework of the water sector is a vital component |
8 |
| |
· enforcement powers must be included in legislation and penalties punitive if they are to be successful | |
| |
· however, it is one of several tools to achieve this and over-reliance on legalistic approaches should be avoided | |
| |
· legislation must be comprehensive but flexible to allow updating as required | |
| |
· the institutional framework of the sector must be covered by legislation | |
Major Elements of Drinking-water Legislation
· Policy Statement· Definition of agencies:
- functions
- responsibilities
- authority
· Source protection, sanitary protection and minimum treatment requirements· Service levels
· Monitoring surveillance
· Water quality standards
· Liability and compliance
· Interim standards and exemptions
Service Levels
· Minimum quantity of water to be supplied
· Continuity of water to be supplied
· Coverage by supplier within their area of operation
· Cost of water supplied
· Penalties required for failure to meet minimum service levels
Source Protection
· Statement of Principles:
- sustainable levels of use
- precedence for use as drinking water
- levels of protection required
· Local scale:
- sanitary completion measures
- abstraction permits
· Regional scale:
- land-use planning
- catchment protection
- groundwater protection zones
- management of water resources
Minimum Treatment Requirements
· Must emphasis the multiple barrier principle· Emphasise the need for all non-community operated piped water supplies to be chlorinated
· Must emphasise the need for adequate record keeping and information sharing
Monitoring and Surveillance
· Identify responsible agencies· Identify acceptable monitoring frequency for all agencies
· Identify reporting mechanism for water quality data
· Identify accepted analytical and quality control procedures
· Describe process of compliance monitoring
Water Quality Standards
· These should not be recorded in the actual water act· Separate legal instrument should be established to allow easy updating
· The basis of standards should be identified
· Priority given to microbiological standards
· Describe process for establishing and reviewing standards
Interim Standards, Compliance and Exemptions
· Interim standards may be required where quality is poor and resources scarce· Better to establish interim standards that have standards which cannot be met
· When setting interim standards, set time limits on them and identify final standard
· Surveillance should assist in achieving standards
· Compliance monitoring sometimes required where there is wilful disregard to meet standards
· Exemptions may be granted where problems are limited by space and time
· Exemptions should be temporary and never set for microbiological standards
Enforcement Powers
· These should be defined in the water legislation establishing the surveillance agency· Legislation should define the protocol or procedures to be followed when enforcement action is undertaken
· Legal penalties must be punitive to be credible and must be achievable in a court of law
· The establishment of legal enforcement powers requires that:
- legislation exists concerning water quality and pollution control- the surveillance agency has specialist legal staff to advise on and initiate legal proceedings
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Establishing National Drinking-Water Standards
Session Objectives
· To describe the need to establish national water quality standards.· To examine the role of the Guidelines as the basis for the development of national standards.
· To discuss the factors to be considered when setting national standards.
· To identify the process of national standards development.
· To identify priorities for national drinking-water quality standards.
· To discuss the establishment of national drinking-water quality standards in the context of legal frameworks.
Introduction
The primary aim of setting national drinking-water standards is the protection of public health and thus the elimination, or reduction to a minimum, of constituents of water that are known to be hazardous to the health of the community. However, standards achieve nothing unless they can be implemented and enforced, and this requires relatively expensive facilities and expertise as well as the appropriate legislative framework.
As reflected in the title, the Guidelines for Drinking-Water Quality are intended to be used as a basis for the development of national standards by the appropriate authorities in Member States. It must be emphasised that the recommended guideline values are not mandatory limits. In order to define such limits, it is necessary to consider the guideline values in the context of local or national environmental, social, economic, and cultural conditions.
The main reason for not promoting the adoption of international standards for drinking-water quality is the necessity of using a risk-benefit approach (qualitative or quantitative) to the establishment of national standards and regulations. This approach should lead to standards and regulations that can be readily implemented and enforced.
The establishment of drinking-water quality standards must follow a very careful process in which the health risk is considered alongside other factors, such as technical and economic feasibility. When establishing national standards, consideration must be given to the practical measures that will need to be taken with respect to finding new sources of water supply, instituting certain types of treatment, and providing for adequate surveillance and enforcement.
National standards will, of necessity be influenced by national priorities and economic factors such as lack of resources for water treatment or unavailability of alternative water supply sources. Such economic factors, conflicting national priorities, and varying local geographical, dietary and industrial conditions may lead to national standards that differ appreciably from the WHO Guideline Values (GV). The final judgement as to whether the benefit from adopting any of WHO recommended GV does or does not justify the risk is for each country to decide. However, considerations of policy and convenience must never be allowed to endanger public health.
The Standards Setting Process
Formulation of standards to protect health usually occurs in two stages, as follows:
(1) The scientific or risk assessment stageThe process for assessment of human health risks associated with exposure to microbial or chemical contaminants is multifaceted and incorporates some of all of the following steps:
- Hazard identification - Utilisation of all available data (epidemiological, animal-bioassay, in vitro, structure-activity relationship) to determine whether an agent can cause an adverse effect in humans;- Dose-response assessment - Determination of the quantitative relationship between the dose and the incidence of adverse health effects;
- Exposure assessment - Estimation of the dose, or level of an agent to which various individuals, or populations are exposed;
- Risk characterisation - Estimation of the incidence and severity of the adverse effects that are liable to occur in a population due to actual or predicted exposure.
At the conclusion of this stage it should be possible to define levels of pollutants that will not result in appreciable health risk in an exposed population.(2) The political and administrative stage, or risk management stage
This second stage is situated in the socio-political and administrative arena and has to cater for a wide variety of sometimes conflicting interests. Risk management usually includes:
- Determination of acceptable risk: to view the problem not as a scientific issue, but rather one of opinion. The judgement of what is an acceptable risk is a matter in which society as a whole has a role to play;- Determination of public to be protected: to consider not only healthy individuals, but also vulnerable population groups;
- Choice of control technology: to formulate a strategy and to select appropriate control techniques;
- Legislation/standards: to consider existing national legal framework and identify necessary legal strategies;
- Economics: to strike a balance between costs and benefits.
The Guidelines have dealt with the scientific stage in the hope that such international risk assessment would provide a sound scientific basis for the further development of national standards.
The risk management stage requires knowledge of the technical, social, financial, legal, and institutional implications of the standards to be adopted, and is more appropriately carried out by national or regional authorities. Those who are involved in setting standards know that at this stage compromises will be inevitable.
Priorities for setting drinking-water standards
(a) The first priority is to make sure that water is available to consumers, even if the quality is not entirely satisfactory. If there is a consideration to discontinue use of a contaminated water supply, there must be provisions made for instituting an alternative water supply.(b) The second priority is to control the microbiological quality of the water supply. The consequences of contamination with pathogenic bacteria, viruses, protozoa and helminths are such that their control must always be of paramount importance.
(c) Toxic chemicals in drinking-water must also be controlled if we are to prevent long-term health effects from exposure to contaminants such as lead, arsenic or certain organic solvents.
(d) Finally, in assessing the quality of drinking-water, the consumer relies principally on the sense organs. Colour, taste, odour and appearance of the water, although not directly related to health, must be acceptable to the consumer. Some countries have elected to issue recommendations, rather than standards, for these aesthetic parameters.
Selection of contaminants for setting standards
There are generally insufficient resources available to deal with all the contaminants that may occur in drinking-water in a country, and it will be necessary to establish priorities. Figure 1 depicts a qualitative prioritisation scheme for setting drinking-water standards. Standards should be set at first for those contaminants that occur frequently and at significant concentrations in drinking-water and that have the greatest health impact. Microbiological contaminants belong to this category.
Figure 1: Priorities for setting
standards
All chemicals are not of equal concern. Six criteria are usually applied in determining the priority chemical contaminants for which drinking-water standards should be first established. These are:
- Severity and frequency of observed or suspected adverse health effects. Of importance are substances that are carcinogenic, and substances which may cause reproductive and developmental effects.- Extent of production and use.
- Ubiquity and abundance of the pollutant in water.
- Persistence in water. Contaminants that resist environmental degradation and accumulate in humans, or in water, deserve attention.
- Exposure from drinking-water relative to other sources such as air or food can be substantial.
- Population exposed. Attention should be paid to exposure involving a large proportion of the general population, and to selective exposures of highly vulnerable groups such as pregnant women, new-born children, the infirm or the elderly.
Legal framework
The format and structure of standards incorporated in legal instruments vary from country to country. However, any regulation will generally contain the following (WHO, 1987):
(a) A statement of the legal instrument, together with a definition of the applicable terms and concepts, specification of the responsible authority, and of the areas and substances to which the instrument will apply.(b) Mention of applicable documents, such as other standards, specification and regulations.
(c) A detailed description of the requirements, including limits on pollutants, applicable tests, mandatory control methods, reporting requirements, etc. Where the requirements are to be implemented over a period of time, a timetable will be included.
(d) A specific statement of the monitoring, reporting, and inspection systems; and
(e) A statement describing applicable penalties for contraventions.
The authority empowered to enact and enforce regulations varies from country to country. As regards drinking-water standards, the appropriate authority may be the Ministry of Health or the Environment.
Compliance with drinking-water quality standards
Once standards are established, it is essential to monitor drinking-water quality to assess compliance with the specified limits and regulations.
Both the water and health authorities are involved in monitoring, the health authority being responsible for ensuring that the legal requirements are met and compliance with standards is achieved.
Monitoring requirements should be appropriate to the needs of the country. They should not be too complicated and cumbersome as this may, from the onset, discourage their implementation.
Both the water and health authorities should have properly equipped laboratory facilities with trained and properly qualified personnel. The water authority is often required to provide event reports and periodic reports of water quality to health authorities, and sometimes to the public.
The water authority, as producer, and the health authority, as overseer, are both accountable for the quality of water supplies.
Conclusion
In developing national drinking-water standards, it will be necessary to take account of a variety of geographical, socio-economic, dietary, and other conditions affecting potential exposure. This may lead to national standards that differ appreciably from the guideline values.
The number of chemical contaminants for which guideline values are recommended is very large. It is unlikely that all of these chemical contaminants will occur in all water supplies or even in all countries. Care should therefore be taken in selecting substances for which national standards will be developed.
In developing national standards, care should be taken to ensure that scarce resources are not unnecessarily diverted to the development of standards and the monitoring of substances of relatively minor importance. Priorities must be established, and this should be done in direct relation to the potential adverse health effects and magnitude of exposure. For instance, in cases where drinking-water contributes little to the overall exposure, standards and other risk management strategies should be directed to media (e.g. air, food) which are important in contributing to total exposure.
The establishment of standards should take into account the possibilities for implementation in view of the socio-economic constraints facing a country.
In all countries, including the richest, choices must be made. The potential consequences of microbial contamination are such that microbiological standards must take precedence over standards for disinfectants and their by-products.
References
National Research Council (1983). Risk assessment in the Federal Government: Managing the process - National Academy Press. Washington, D.C.
World Health Organization (1987). Setting environmental standards - Guidelines for decision making. Geneva.
Presentation Plan
|
Section |
Key Points |
OHP | |
|
Introduction |
· aim of setting national standards is to protect public health. Standards must be implemented and enforced through legislative framework |
1 | |
| |
· the WHO Guidelines are intended to be used as a basis for establishing national standards | | |
| |
· it is not considered appropriate to set international standards | | |
| |
· national standards must consider national priorities, economic factors, technical feasibility and health risk. | | |
| |
· these will vary between Member States | | |
|
The standard setting process |
· this is done in two stages: |
2 | |
| | |
1. scientific or risk assessment stage - 4 steps - largely dealt with by the Guidelines |
|
|
| |
2. political and administrative stage - 5 factors to be considered - to be carried out by national/regional authorities | |
|
Priorities for setting drinking-water standards |
· there are four priorities for standards: |
3,4 | |
| | |
1. unrestricted availability of water to consumers | |
| | |
2. control of microbiological quality of water supply | |
| | |
3. control of toxic chemicals | |
| | |
4. aesthetic standard of water | |
|
Selection of contaminants for setting standards |
· resources are the limiting factor to deal with contaminants, therefore priorities need to be set based on frequency and concentration of occurrence and health risk. Microbiological contaminants are a priority |
5 | |
| |
· six criteria have been identified to prioritise chemical contaminants. | | |
| |
· when setting standards, need to establish costs of meeting standards, current water quality status and resources available to meet national standards | | |
|
Legal framework |
· format and structure of standards in legal instruments vary between countries but generally have 5 common components - |
6 | |
| | |
1. statement of the legal instrument | |
| |
|
2. mention of applicable documents | |
| | |
3. detailed description of the requirements | |
| |
|
4. statement of the monitoring, reporting and inspection systems | |
| | |
5. statement of penalties for contraventions | |
|
Compliance with drinking-water standards |
· to ensure compliance with standards the quality of the drinking-water must be monitored by the appropriate bodies |
8 | |
| |
· monitoring regime must be appropriate to the country's needs |
| |
|
|
· monitoring requires adequate equipment and trained personnel |
| |
|
Conclusion |
· drinking-water quality standards may vary nationally due to differing conditions and may be appreciably different from guideline values |
| |
|
|
· GVs are recommended for a large number of chemical contaminants and not all are applicable to every country | | |
| |
· countries must prioritise substances to develop national standards. These should take into account health risks and magnitude of exposure primarily, as well as resources to ensure implementation | | |
National Water Standards
· Aim to protect public health· Must be achievable and enforceable
· Should reflect national conditions and priorities
· Set for:
- quantity of water supplied
- continuity of supply
- coverage of the population
- cost of water
Formulation of Standards
Scientific or Risk Assessment Stage
· Hazard identification
· Dose-response assessment
· Exposure assessment
Political/Administrative Stage of Risk Management Stage
· Determination of acceptable risk
· Determination of public to be protected
· Choice of control technology
· Legislation/Standards
· Economics
Four Priorities for Standards
· Unrestricted availability of water to consumers
· Control of microbiological quality of water supply
· Control of toxic chemicals
· Aesthetic standard of water
Priorities for Evaluation
Selection Criteria for Setting Standards
· Severity and frequency of observed or suspected health effects
· Extent of production and use
· Ubiquity and abundance of pollutant in water
· Persistence in water
· Exposure from water relative to other sources
· Population exposed
Framework for Drinking-water Quality Standards
· Statement of legal instrument
· Mention of applicable documents
· Detailed description of requirements
· Statement of monitoring, reporting and inspection systems
· Statement of penalties for contravention
Standard Setting Process
Categories for FaecalColiform Densities
|
Category |
Faecal coliforms/100ml |
Health Risk |
| |
| |
|
A |
0 |
No risk |
|
B |
1-10 |
Little risk |
|
C |
11-50 |
Intermediate risk |
|
D |
>50 |
High risk |
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Human Resources
Session Objectives
· To describe the human resource requirements of monitoring programmes, whether quality control or surveillance, for all levels of staff.· To highlight the need for a broad approach to human resources development, including career development structures, overall staffing and training.
· To emphasise the need for and value of ongoing investment in staff in terms of training, delegation of responsibility and encouragement to join professional bodies and undertake applied research.
· To briefly describe some key responsibilities of managerial, analytical, field and data management staff.
Introduction
Monitoring programmes are reliant on good human resources to make them efficient and effective. The strength of any monitoring programme is determined by the weakest element and this can often be identified as inadequate human resources. This may result from insufficient numbers of staff, but also from insufficiently trained and motivated staff who feel undervalued and do not perform their duties well. It is therefore essential that human resources development strategies are developed for the surveillance agency and quality control staff within water supply agencies to ensure that they have the capacity and capability to carry out the activities assigned to them.
Human resources development strategies are not merely training programmes, they encompass a wider view of staff development which acknowledges that access to career structures, interaction with peers and ongoing professional development are all of equal value. Furthermore, the human resources development strategy for an institution should also address the need for adequate numbers of staff at different grades and within different wings of the institution and the need to focus recruitment purely on the basis of job requirements. Therefore, all these elements should be covered by the human resources management team in the monitoring agencies.
Staffing requirements
Different countries will have different staffing requirements depending on the stage of development of monitoring programmes, the institutional framework of the water sector and the availability of qualified and trained personnel. However, appropriately qualified and trained staff will be required both in the surveillance agency and the quality control wing of the water supply agency.
Staff in both agencies will fall into four broad categories: managerial staff; analytical staff; field staff; and, data processors/managers. However, it should be recognised that this classification is very broad and that clearly there will be many instances when individuals play more than one role. For instance, it may be common to find that field staff also undertake analytical work, or that managerial staff or analytical staff undertake a significant amount of information management. Thus the descriptions provided below of key tasks relate to generic needs of the position rather than to the specific tasks undertaken by individuals.
Managerial staff
Managerial staff are responsible for the overall planning, operation and monitoring of the programme. They take responsibility for strategic developments in the programme, reorientation to meet new or changing objectives and for the overall staffing and human resources development of the programme. Managerial staff will certainly include the overall programme or section manager and head of the laboratory/analytical services and possibly other staff such as the head of the information management unit. However, the programme manager and head of analytical services are possibly the two key members of staff and are discussed in more detail below.
Programme manager
The role of programme managers in both supply agency and surveillance agency will be to co-ordinate activities of the different sections and bear ultimate responsibility for the water quality data produced. Both should bear administrative responsibility for their programmes and the staff within the programme. This will include assessing training requirements in collaboration with other senior staff, defining training programmes, lobbying for resources and establishing staff development strategies. They should both clearly identify research needs within their organisation. As both will take ultimate responsibility for the quality of data their organisations produce, both need to work closely with the quality assurance officer to ensure that the analytical data produced is reliable.
In both agencies, the programme manager should lead the national planning team defining monitoring programmes and should ensure that regional and local level monitoring programmes are consistent with broader national goals. The programme mangers will also be expected to lilies with section heads to ensure that adequate standard operating procedures are prepared and followed through all stages of the monitoring process from sample collection, through analysis to data manipulation. They should also ensure that data are distributed to all key institutions within the sector in a comprehensible format. Where feasible, programme managers should also take responsibility for ensuring public access to water quality information through the publication of annual reports on water quality.
Other responsibilities will vary between the two agencies. Within the water supply agency, the programme manager must be responsible for the reporting of data to the surveillance agency and liaison with the surveillance agency in cases of water quality failure. They should also make both the operational and senior management staff immediately aware that a water quality failure has occurred and suggest remedial and preventative action.
Within the surveillance agency, the programme manager should co-ordinate enforcement action taken against water suppliers and should be responsible for initiating legal actions where these are to be undertaken. In some circumstances, as the person bearing ultimate responsibility for the water data, the programme manager should act as the expert witness in cases of water quality failure, although this may also be the responsibility for the head of analytical services.
The importance of good senior management in monitoring programmes cannot be overstated. It is vital that senior managers understand the programme and pressures staff face and be sympathetic to their needs. Good direction and an active interest in the staff is vital for the success of the programme.
Head of Analytical Services
The Head of the Analytical Services is another key member of the senior management team of monitoring programmes and much of the routine operational management of laboratories, sample collection and reporting of data should come under the remit of the Head of Analytical Services. Clearly a fundamental role of the Head of Analytical Services is to ensure that the reporting of analytical results is done in a comprehensible and timely fashion and in the event of a water quality failure should immediately alert the programme manager.
Key responsibilities will include writing standard operating procedures and ensuring that they are followed by all analytical staff in the laboratory. This member of staff should also actively liaise with the quality assurance officer and when problems are identified in the quality of data produced, should follow this up and identify the cause of the quality failure and implement steps to rectify the problems in the shortest possible time frame.
The Head of the Analytical Services will also be expected to ensure that all the necessary equipment and consumable are available to carry out comprehensive analysis of water quality on both a routine and non-routine basis and have budgetary control of the laboratory services. They should also ensure that adequate health and safety procedures are in place and fully understood by all staff working within the laboratories. As head of section, they will be expected to monitor and evaluate staff performance and identify training needs and appropriate training opportunities.
Other Managerial Staff
The other managerial staff within the programme will depend on the size and structure of the programme, but may include information management, legal advice or administration. All these are key roles, but which may be carried out by other staff members as part of their responsibilities so no further detail will be discussed here.
Analytical, field and data management staff
The bulk of the technical staff employed on a monitoring programme will be involved in the collection and analysis of samples and the processing of analytical data. Some duties of the staff will overlap between several roles, therefore a member of staff who undertakes analysis may also be responsible for sample collection or data management etc. It is essential that staff are recruited who have the necessary skills and experience to do the job they have been given and receive ongoing training whilst in post.
Analytical staff
The analytical staff will report to the Head of the Analytical Services, either directly in the small programmes or through section heads in larger programmes. Analytical staff will normally be divided into chemical and microbiological sections and possibly have further subdivisions depending on the scope of the programme and the size of the analytical facilities. In some countries, sections will also include biological monitoring and sub-division of chemistry into wet chemistry, organics and trace metals etc.
It is essential that each section has at least one degree educated analyst who can supervise the analysis of other members of staff. Much of the analysis may actually be done by technicians with a lower level of education, but who have experience of routine analysis. They will be commonly supported by assistants who effectively learn whilst in post. It is important that the laboratory has sufficient analysts to perform the numbers of analyses required for routine and non-routine investigations of water quality, but that it is not overstaffed. Underemploying staff tends to lead to motivation problems and boredom and may lead to a loss of good staff.
A check list of key activities is given in box 1 below.
|
Box 1: Check list of laboratory staff activities · Routine and non-routine
analysis of water quality |
A key member of the analytical staff is the quality control/assurance officer who is responsible for ensuring that the quality of data produced by the laboratories is acceptable and who reports directly to the most senior member of staff. This member of staff will have to monitor analytical and field work, prepare and submit blank samples to analysts and carry out audits of all documentation, including methods, SOPs and field and laboratory notebooks, to ensure that information provided is correct and complete.
Good quality control is essential for monitoring programmes to maintain credibility in their results. It is often a false economy not to recruit a QA officer on financial grounds as the lack of demonstrable quality assurance and control may result in limited ability for water suppliers or regulators to perform effectively.
Where financial constraints prohibit the recruitment of a specific quality assurance officer, a member of staff may be nominated as QA officer, although this will require that this persons work is also monitored by a fellow staff member. In these circumstances, it is important that senior staff minimise conflicts of interest.
It is important that all analytical staff are aware of and follow the standard operating procedures and keep a clear record of all operations performed. They should be actively involved in the quality control/assurance programme and understand its value to them as analysts in improving techniques and maintaining high standards.
Field staff
In some programmes, field staff are specifically employed for the collection of samples and carrying out field tests so a restricted number of parameters. In other programmes, these roles are performed by the analytical staff. Where field staff are employed, it is essential that they have sufficient skills to be able to perform the activities assigned to them and an understanding of the wider implications of their role.
Training should be provided in standard operating procedures for sample collection, storage and transport and the proper labelling of samples and the information to be included when sending samples. It is essential that sampling procedures are designed to be representative of water quality and that field staff have an appreciation of the risks and implications of sample contamination. Field staff should also be clearly aware of the handling procedures for any preservative agents which may be used when transporting samples.
Where field staff will carry out some basic analyses on-site, they obviously require adequate training in the techniques to be employed, recording of the results and interpretation of the data. Such on-site analyses may include pH, chlorine residual, thermotolerant (faecal) coliform analysis and conductivity. In some circumstances, field staff will be expected to make recommendations for actions based on water quality data, particularly when they are dealing with community managed rural water supplies in remote areas. It is essential that these staff are provided with the skills to do this effectively.
A key role field staff should undertake is sanitary inspection and risk assessment of water supplies and sources. This data may be used by themselves to implement remedial or preventative actions, but should also be submitted to the central or regional data store. Again, field staff will require training in appropriate techniques and in the interpretation and use of data generated. A check list of key activities for field staff is given in box 2.
|
Box 2: Check list of field staff activities · Sampling of water supplies and
sources |
Information management staff
Information management staff are responsible for the collation and manipulation of all data generated in monitoring programmes. They should process data into standard reporting sheets and produce regular water quality reports.
Information management may be done by a member of the analytical staff who takes responsibility for data processing. This is acceptable when the throughput of data is limited and where only standard analytical reports are being produced. However, this approach limits the use of the data and serious consideration should be given to appointing a full time information management system administrator who can produce and manage a national water quality databank and produce summaries of water quality data for the general public or other agencies. There are many uses of water quality data and effective management of available information can greatly enhance national decision-making regarding priorities for investment and selection of appropriate alternatives.
Staffing structure
It is important that all monitoring programmes, whether quality control or surveillance, have a staffing structure which clearly defines lines of responsibility and accountability and which provides a framework for career development within the programme. Each monitoring programme will be structured in slightly different ways, but in many circumstances, a clear demarcation of roles played by the enforcement wing of the water quality department and the analytical wing is established.
In all organisational structures, it is essential that there are clear lines of accountability and responsibility which allow senior managers to run departments and programmes effectively. Usually, if programmes are to be successful, there should be a high degree of delegation to senior staff and regular meeting of senior management to discuss progress.
Delegation of key responsibilities allow staff to feel that they have a greater investment within the programme and more closely identify with the programme's success or failure. However, it is important that delegation is not seen as abrogation of responsibility by the programme manager, who must retain an overall responsibility for the performance of the programme.
Training and professional development
Training of staff will be essential in most circumstances. Although staff should be recruited with appropriate qualifications, apart from the senior staff, they may have limited professional experience. Therefore, training in the aims and objectives of the programme, use of equipment and quality control procedures will have to be given. Ongoing training will also be required in safety and other aspects, such as data processing. Training should be focused on the needs of staff and aim to assist them in optimising their performance. However, it is also valuable to provide staff with opportunities to acquire new skills and develop into new areas of activity as this will help to motivate staff. If this is done, it is important that staff are able to use new skills developed during training within the workplace. This is important as otherwise these skills may be rapidly lost without practice and because restricting potential to take new areas of responsibility and put theory into practice may well lead to frustration amongst staff.
Training programmes may be either established as in-house programmes utilising resources within the agency or programme, or may involve outside agencies. In-house training is only likely to be cost-effective where very large numbers of staff will require similar training and therefore is possibly most appropriate for training in analytical techniques or sanitary inspection or as part of an orientation programme. In-house training is less likely to be able meet all the ongoing professional needs of individuals and in these circumstances outside courses should be used.
In addition to training, staff should also be encouraged to undertake applied research, attend conferences and seminars and join professional bodies as means of improving professional knowledge. Training should also be linked to a broader process of improvement which encourages progression on the basis of merit and provides a career structure for staff. Unless this is done, staff-turnover will be high and motivation low.
Conclusion
Human resources are a key element in the success or failure of monitoring programmes to meet their objectives. Without an adequate strategy to develop the human resources available and attract high calibre staff, monitoring programmes rapidly stagnate. Whilst poor quality of staff in water quality monitoring programme may reflect a wider difficulty in attracting staff to the sector, every effort should be made to invest in staff at all levels.
Human resources development should encompass a much wider remit than training and should address issues such as career structures and professional development. It should also provide all levels of staff with the support and framework within which to function effectively and efficiently.
References
Bartram, J. Resources for a Monitoring Programme, in Bartram, J. and Ballance, R. (eds) Water Quality Monitoring, 1996, Chapman and Hall, London, pp 61-70.
Howard, G. National Water Analysis Laboratory, Zimbabwe, Report 7, ODA Project Report, 1996.
Mtetwa, S., Howard, G. and Jackman, R., Strategic Plan for the National Water Quality Inspectorate and the National Water Quality Analysis Laboratory, Paper for the Management of Change Task Force, department of Water Resources, Zimbabwe, 1996.
Presentation Plan
|
Section |
Key points |
OHP |
|
Introduction |
· monitoring programmes are reliant on good human resources |
1 |
| |
· need to have human resources development strategies in surveillance and supply agencies | |
| |
· HRD strategies are not merely training programmes but should address wider issues such as staff numbers, career structures and pay scales |
|
|
|
· recruitment should be focused on need for staff | |
|
Staffing requirements |
· these vary according to level of development of monitoring programmes, institutional framework and availability of staff |
2 |
| |
· staff may be divided into 4 categories: managerial; analytical; field; and data processors | |
| |
· many staff may have roles which overlap more than one area |
|
|
Managerial staff |
· responsible for planning, implementation and monitoring of programmes |
3,4 |
| |
· should also be responsible for strategic development of programme |
|
|
|
· will include programme managers and other key senior staff such as head of analytical services/laboratory | |
| |
programme manager | |
| |
· bear ultimate responsibility for data quality in their institution | |
| |
· responsible for overall administration of programmes and need to work closely with heads of section and QA officer | |
| |
· need to ensure that monitoring programmes conform with national goals and that data is distributed to appropriate agencies | |
| |
· in the supply agency, the manager should ensure that information sent to surveillance agency in timely manner when failure in quality occurs | |
| |
· make operational and senior staff immediately aware of water quality failure & suggest remedial/preventative action |
|
|
|
· surveillance agency: co-ordinates enforcement action and for initiating legal action when required | |
| |
· may also act as expert witness | |
| |
· good senior management is essential for smooth running of programmes, good direction and active interest in staff vital for success of programme | |
| |
head of analytical services | |
| |
· responsible for routine operation of laboratories | |
| |
· must ensure data reporting is in a format which is comprehensible and done in a timely fashion | |
| |
· immediately alert programme manager in the event of water quality | |
| |
· should prepare SOPs and ensure that these are followed by all analytical staff | |
| |
· ensure that health & safety procedures in place | |
| |
· ensure that laboratories are able to carry out all routine and non-routine analysis requested by programme manager and that is consistent with programme goals | |
| |
· also identify staff training needs and evaluate staff performance |
|
|
Analytical, field and data management staff |
· bulk of staff involved in the collection and analysis of samples and processing of data produced |
5,6,7 |
| |
· individual staff members may have roles which overlap more than one area, therefore essential they have the skills to perform all tasks assigned |
|
|
|
analytical staff | |
| |
· normally divided into two or more sections according to discipline | |
| |
· each section should have at least one degree educated member of staff as a supervisor, although analysis may be done by technicians | |
| |
· technicians may be supported by assistants who learn in post |
|
|
|
· need sufficient analysts to perform analysis required, but should not overstaff laboratories as this will lead to under-employment and a possible loss of motivation | |
| |
· check list of key tasks is given | |
| |
· key analytical staff member is the QA officer as they are responsible for ensuring that data produced is of an adequate quality | |
| |
· should monitor use of SOPs, submit blank samples, audit documentation and reports to most senior member of staff | |
| |
· where specific QA officer cannot be recruited, then appoint a member of staff to do this in conjunction with other roles, but ensure that conflicts of interest are minimised and that QA officers work is also monitored |
|
|
|
field staff |
|
|
|
· may have specific field staff employed to collect samples and undertake on-site analysis | |
| |
· staff should be trained in sample collection, storage and transeport and be aware of their role in the monitoring programme and the need for quality control in sampling | |
| |
· where on-site analysis is carried out by field staff, training will also be required in this | |
| |
· field staff should also be effective communicators, particularly where they are providing feedback to communities and initiating remedial and preventative actions | |
| |
· field staff should also undertake sanitary inspection and risk assessment of water sources | |
| |
information management staff | |
| |
· responsible for input and manipulation of data and generation of water quality reports | |
| |
· analytical staff may undertake some data processing, although this limits use of data and consideration should be given to appointing a full time member of staff | |
|
Staffing structure |
· all programmes should have a staff structure which shows clear lines of responsibility and accountability | |
| |
· structure should also provide a framework for career development |
|
|
|
· enforcement and analytical wings in a monitoring body should be clearly separated | |
| |
· delegation is important, but should not be allowed to become abrogation of responsibility | |
|
Training and professional development |
· training is essential in most circumstances, including for staff with high qualifications |
8,9 |
| |
· training will include programme aims and objectives, SOPs, QA procedures etc. | |
| |
· staff should also be provided with an opportunity to acquire new skills, however, it must be possible to practice these in the workplace to maintain motivation | |
| |
· training may be either in-house or use external trainers |
|
|
|
· in-house training only cost-effective in large programmes where many staff require the same training at one time | |
| |
· otherwise make use of training opportunities outside the programme which may be more focused on individual needs | |
| |
· staff should also be encourage to undertake applied research, attend conferences and join professional bodies | |
|
Conclusions |
· human resources are vital to monitoring programme to meet objectives | |
| |
· HRD strategy is essential and should address training, career structures and ongoing professional development | |
| |
· monitoring programmes must be able to attract and retain high quality staff | |
Human Resources Development: Constraints
· Lack of adequate numbers of trained staff is often a key constraint· Training should be ongoing and for all levels of staff
· Training opportunities are often limited
· Training must be matched to job requirements and likely future development of staff
· Training needs assessment is vital for human resources development
Staffing Requirements
· This depends on:
- size of programme
- frequency of sampling
- numbers of samples
- whether on-site or laboratory testing used
· In a microbiology laboratory doing 70 samples per day by membrane filtration (or 40 by MPN):
- 2 laboratory staff (1 scientist, 1 technician)
- 2-3 (minimum) field staff
- 1 (possibly) data processing staff
· Using field testing approach:
- 16 samples per day can be processed
- Therefore up to 16 point sources or 1-3 piped water supplies may be visited per day
· Provincial and national levels:
- staff to collate information, provide feedback & identify trends
- these may not be full-time posts
Managerial Staff
Programme Manager
· Responsible for planning and management of monitoring programmes· Make sure programme conforms with national goals for the sector
· Water supply agency: liases with surveillance agency and makes sure data is shared
· Water supply agency: ensures remedial action taken promptly
· Surveillance agency: responsible for enforcing relevant legislation
· Surveillance agency: liasing with suppliers to help improve water supply quality
· Both provide direction and leadership and oversee staff development
· Both receive QA data from QA officer and take ultimate responsibility for data
· Oversee information dissemination, staff development and QA
Head of Analytical Services
· Responsible for routine operation of laboratories and for quality of data produced· Should report findings in a comprehensible and accessible format
· Should alert programme manager when results indicate water quality failure
· Should develop SOPs and ensure these are followed
· Should ensure health & safety measures are in place and observed
· Should identify staff training needs and evaluate performance
Analytical Staff
· Usually divided into sections by discipline· Each section should be headed by a degree educated supervisor
· Much of analysis may be done by technicians
· QA Officer is vital to ensure that results produced are reliable
· QA Officer reports to most senior staff member - usually programme manager
Field Staff
· May collect samples and/or carry out on-site testing· Important to provide field staff with adequate training and support
· Field staff must be effective communicators, particularly where community supplies are monitored
· Field staff should undertake sanitary inspection and risk assessment
Information Management Staff
· Responsible for input and manipulation of data· Maybe dedicated member of staff or member of analytical staff
· Must have support to maintain software and hardware
· Must be trained in use of appropriate software and understand basic data manipulation
Human Resources Development: Training
· Training should be provided in a number of ways, including:
- short courses
- 'on-the-job'
- longer formal training
· Refresher training is vital for ongoing good operational performance· Senior staff should respond to training needs of their staff and identify suitable opportunities
· Training is not the only means of acquiring additional knowledge & expertise
· Applied research has great value for HRD
· All training should be linked to career development
· Training should be evaluated
Example of Human Resources
Development for Water Supply Surveillance
Source: Lloyd et al, 1991
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Cost Recovery
Session Objectives
· To highlight the need for cost recovery by some mechanisms in the water sector to ensure sustainability and to highlight the consequence of under-investment in water supply.· To describe some of the commonly used mechanisms for recovering costs, including the use of tariffs and subsidies.
· To describe some common charging policies and highlight the need to implement charging mechanisms which promote both universal coverage and the rational use of water.
· To highlight the need to keep water charges affordable and to highlight the dangers of disconnection policies for public health.
Introduction
The production and provision of clean water to consumers entails a cost both in terms of initial capital outlay and in ongoing operation, maintenance, management and extension of services. However, because of poor planning for cost recovery, a lack of government funding and inadequate tariff rates, the ability of the sector to recover costs is often limited even for routine operation and maintenance. This has led to problems in providing sustainable water supplies.
Cost-recovery and application of water charges is a very political issue as many consumers have been used to provision of water supply as a free service or one for which only nominal payment is made. There is still a widely held view (in developed countries as well as less developed countries) that water is 'free' and that water supply should remain a free social service.
To a certain extent this concept is correct in that if a person wishes to collect untreated water they can often do so at no cost, apart from their time and potentially their health. However, water supply treated so as to represent no health risk, is not a free service and the cost of water supply largely reflects the 'added value' cost of treatment and delivery.
It is essential for long-term sustainability of the sector that costs are recovered by some mechanism, whether through application of full cost-based charges to consumers or by Government support to the sector. Where cost recovery and sector funding has been ignored, the effect has been a deterioration of infrastructure which eventually leads to the breakdown of systems, absence of an adequate water supply and an increased public health risk. It is also important to recognise that costs for treatment and disposal of return flows of wastewater must also be recovered for the sector to be sustainable.
It is essential that the profile of the need to pay for water supplies amongst consumers is maintained at a high level. Unless consumers are convinced of the need to pay for services, cost-recovery will remain problematic and the long-term sustainability of the drinking water provision will be compromised. However, this also means that service quality needs to be sufficiently good to encourage payment and that water suppliers are seen to be responsive to the demands of consumers.
Consequences of poor cost-recovery
In many countries, the issues of cost-recovery and sector sustainability were ignored for a long period. As a result, tariffs set were unrealistic and frequently there was insufficient Government subsidy to make up the shortfall in the costs of the service provided. In consequence, the infrastructure has deteriorated and service quality has declined. This process is outlined in figure 1 below.
Inadequate cost-recovery, will result in an inability to operate and maintain existing supplies properly with consequent increased of leakage, water supply interruption and likely deterioration in both the quality and quantity of the water supplied. This will lead to increased public health risks, a likely increase in morbidity and mortality rates and an increased burden on the health care system.
Inadequate cost-recovery will also result in an inability to extend water supplies to unserved areas, thus continuing a cycle of inequitable access to water supplies. This not only fails to satisfy the basic human right of all peoples to have access to an adequate water supply (UN, 1977), but will continue to place a continued extra burden on the health care system. It is vital that sufficient resources are raised from existing water supplies not just to ensure their continued functioning, but also to extend services to the urban and rural populations who lack access to an adequate water supply.
A good example of this is the water supply in Lusaka, Zambia, where a prolonged lack of investment has led to an almost complete breakdown of existing services and an inability to extend services to serve new settlements within the urban conurbation. As a result, only in the region of 30 per cent of the population are connected to a water supply, although the figure for coverage with an adequate, continuous water supply is far lower.
The protection of the water resource base is a key factor in water supply and where revenue generated has been insufficient to cover the costs of treatment of wastewater, water resources are likely to become at risk from pollution. If poorly or untreated wastes are discharged into streams or excessive leakage of waste to groundwater is allowed, then this will lead to a deterioration in natural water quality. This has two principal effects: firstly it increases the treatment requirements for the production of drinking water and therefore increases the cost of water supply; secondly, if pollution is allowed to continue and where certain pollutants (such as aromatic hydrocarbons) are present there can be a long-term loss of resources resulting in the need to develop new, possibly less accessible, water resources.

Figure 1: Consequences of poor
cost-recovery
Recovering costs
Costs are usually recovered, at least in part, through the levying of a charge on consumers by the supply agency. A certain proportion of the costs may be recovered directly from Government. However, increasingly the sector is expected to be self-financing with limited support and water suppliers are expected to raise funds for on-going costs and to raise sufficient funds for major rehabilitation and extension works.
In many countries there is now a political decision that the subsidisation of social services will no longer be carried out and the water supply sector is expected to become self-sustaining in a very short period of time. This may have grave consequences for public health as water suppliers increase tariffs in order to recover costs and new policies, such as disconnection, are enacted. In these conditions, plans for extending water supplies to unserved areas are often shelved and low-income areas risk to disconnection for non-payment of bills.
An important factor in cost-recovery is the setting of adequate standards of service. It has been shown that consumers are willing to pay for good quality services and are prepared to pay increased costs for improved services in terms of water quality and supply continuity. However, where water supply services are poor, the collection of revenue is difficult and costs are rarely recovered. In some situations, consumers may be willing to be disconnected from a water supply whose service quality is poor and whose costs are high. This leads to a fundamental question of water supply improvement: does service quality improvement or cost-recovery improvement take priority and therefore should tariffs be raised in order to improve service quality or should service quality be improved to allow increased revenue to be collected?
Many water suppliers argue that in order for them to raise the capital required to improve service quality, tariffs which reflect the cost of doing this need to be charged immediately. Once sufficient revenue is collected then service improvements can be implemented. However, from a public health point of view, it is vital that service quality improvement in areas where this is poor, should be implemented immediately. There is a significant risk that users will be willing to disconnect themselves from an expensive but poor quality service rather than pay what they see as unrealistic prices. This will inevitably lead to greater health risks as unprotected water sources are used for water supplies.
Another significant risk arises from the shift towards user-only funding of the water supply sector is that it will continue to marginalise the poor in unserved areas. These users will continue to rely on poor quality water supplies unless some form of subsidy is made available to support the provision of services to them. Furthermore, these sections of the population are also frequently forced to pay higher unit costs for drinking water from vendors where no connection to some form of centralised water supply is made available.
Where Government subsidies the supply of water to poorer sections of the community, it is important that some element of household payment, however nominal, is retained to encourage responsible use of water supplies and infrastructure. It is also important that all users of the water supply pay for the services that they receive. In many countries, the worse defaulters on payment of water bills are Government Institutions, the military and the wealthier sections of society. In many countries, low-income groups actually subsidise the high-income groups.
The need to pay for drinking water supplies should remain a high profile issue nationally. Promotional campaigns on payment and the implications for service quality in the event of nonpayment and clearly described and the link between payment of fees and improving water supplies should be clearly shown. In some cases, water suppliers provide annual statements of water supply quality and expenditure. These allow consumers to be able look at how their money has been spent and what improvements that has led to. Water suppliers and surveillance bodies should be proactive in their efforts to raise the profile of the need to raise revenue and the responsibility of all consumers to pay bills.
Charging policies
Charging policies can be established in a number of ways. The key principle of charging policies however, should be to ensure that water supply remains accessible for all consumers whilst still recovering overall costs of the water supply. Charging policies should be established which are fair and equitable, provide incentives to conserve water and are simple and comprehensible to consumers.
The tariff set will depend on the determination of costs and the ability and willingness of consumers to pay. Consideration should be given to whether a pay-for use system is employed or a rates system used. Pay-for-use systems require household water meters to be installed to gauge individual household consumption, whereas rate systems rely on estimation of property value and the use of bulk meters to determine bulk demand. If a flat rate system is employed it is essential that consideration be given to how excessive consumption will be dealt with and whether fines for consumption of a certain level of water will be introduced.
Often a mixture of flat rate and pay-for-use systems are used to set tariffs. These systems generally employ low flat rates for a given amount of water per household and thereafter use a progressive rate for increasing water use. The advantage of this system is that it provides some security to the poor as low rates of water use are inexpensive, whilst allowing wealthier members of society use the water they require and also allows transparency of charging.
The problem with this system is the determination of the maximum allowable supply charged at a flat rate. A number of solutions have been employed. At the most basic level, an equivalent of 5 litres per capita per day can be used as the water required for consumption and this may be used as the flat rate maximum. However, in most countries where combined tariff systems are in place a flat rate is used which includes sufficient water for all basic domestic use, which will raise this figure to about 30-50 litres per capita per day.
This approach can be implemented using a block rate system or a step rate systems. The step rate system employs progressively higher charges for bands of consumption. Thus the initial band will be a volume sufficient for basic domestic needs and charged at the minimum rate. Increased consumption therefore brings a penalty of a higher unit charge, which increases in a series of steps. The principle of this method is to encourage conservation of water and to penalise those who use excess amounts. Block rates work in the reverse, with the maximum rate charged for volumes sufficient for all domestic use and thereafter low unit charges for increased consumption with minimum charges for very high consumption. This works on the principle that although unit charges decrease, as the number of units consumed increases, sufficient revenue is generated.
Keeping water charges affordable
It is essential that water charges remain affordable for all consumers, this may be achieved through employing cross-subsidisation techniques. Cross-subsidisation allows different tariffs to be set according to the ability to pay of different groups of consumers. The principle is that richer consumers pay an increased proportion of costs in order to ensure that poorer consumers can afford their water bills. Cross-subsidisation can be an effective mechanism for ensuring that costs charged reflect ability to pay. However, it is frequently contentious, difficult to implement and requires careful and detailed planning if it is to be successful.
One way in which costs can be reduced is to encourage greater community or consumer involvement in operating and maintaining the supply. This is an approach commonly used in less developed countries. However, with sophisticated systems utilising treatment plants and an in-house level of supply, it is much more difficult to rely on community involvement to reduce costs because specialist skills and a large amount of time are required.
Careful consideration should also be given to whether domestic water bills should be the same as industrial water charges. Industry uses a great deal of high-quality water and this forms part of its raw materials. As industry uses a large amount of water and as it is essentially profit making in most circumstances, there is much to be said for subsidising domestic water tariffs through application of higher rates to industry. This is further strengthened by the fact that industry accounts for a great deal of the pollution of water resources and thus directly contributes to increased treatment costs.
Agricultural water use is generally covered by the water resource management body, although there needs to be close liaison to ensure that farming activities do not pollute water sources used for drinking water supplies and that priority for use as drinking water is always maintained.
The difference between in ability to fully recover costs in rural and urban areas must also be considered. There is greater potential for revenue collection in urban areas where there are more people living in restricted surroundings. In rural areas, the low density of population often makes full cost-recovery difficult. In these circumstances the possibility of subsidising rural water supplies by urban consumers should be considered.
One aspect of cost-recovery which is often difficult to address is the funding of surveillance activities undertaken by watchdog bodies. In most situations this activity is funded from local or national government through taxing of the population. This approach is workable as long as there is a sufficient tax base to raise revenue for all the competing demands. However, in many countries such funds are not available and water suppliers must contribute to the funding of a watchdog body.
Non-payment issues
The issue of non-payment of water charges is an issue which provokes considerable debate and great care must be taken when dealing with non-payment issues to ensure that public health is not unacceptably compromised.
Many water suppliers insist that policies of disconnection in cases where there is continued nonpayment of bills are essential if revenue collection and hence cost-recovery is to be maintained. However, it should be stressed that there is no evidence of significantly increased levels of nonpayment of bills where there is no threat of disconnection. It should also be stressed that disconnection from a public water supply represents a significant health risk to the whole community and not just the disconnected household. Significant increases in disease are noted in areas where disconnections have taken place.
In many areas where disconnection is heavily promoted, water supplies have been privatised. In these circumstances, disconnection may be more related to profits of the company rather than inability to recover costs. There are real dangers in disconnecting users from water supplies and it is not method that can be recommended because of the public health risk.
Where household resource are limited and non-payment becomes problematic, other solutions should be identified. These may include a minimum amount of water provided effectively free of charge, employing large scale subsidisation from wealthier domestic users and industry or installing flow limiters on households with a history of persistent non-payment.
Conclusion
Cost-recovery is vital if water supplies are to sustainable and if they are to meet future demands. It is important that the revenue raised covers operation and maintenance costs and generates capital for extension and rehabilitation of water supplies.
Some element of subsidy is often required, whether from Government social funds or through the application of differential tariffs for low and high income residential areas and differential tariffs for domestic and industrial water users.
Disconnection policies represent a significant health risk which is likely affect the wider community and not just those disconnected. Disconnection of households from piped water supplies for non-payment of bills can never be justified from a public health standpoint and such policies should not be enacted.
References
OFWAT (1993) Annual Report 1992. HMSO. London.
Robens International Centre for Public and Environmental Health, Water and Health, Paper Presented at the Institution of Civil Engineers-Royal Institute of British Architects Meeting Who is Making Britain Sick?, 1996.
U.N. (1977), World Water Conference, Mar del Plata, Argentina,
WHO (1990), Handbook of Financial Principles and Methods, World Health Organization Working Group on Cost-Recovery. WHO/CWS/90.10.
Presentation Plan
|
Section |
Key points |
OHP |
|
Introduction |
· production and provision of clean water has both capital and ongoing costs, it is not free |
1,2 |
| |
· poor cost recovery leads to inability of the water sector to meet the demands placed upon it | |
| |
· cost-recovery is often contentious, but is essential |
|
|
|
· costs may be recovered from Government, from consumers or through a mixture of both | |
| |
· where water charges are levied, quality of service must be good and reflect charges made | |
|
Consequences of poor cost-recovery |
· cost-recovery has been ignored by some countries and so tariffs were too low and government subsidy insufficient to make up shortfall |
3,4 |
| |
· in consequence, infrastructure has deteriorated and service declined | |
| |
· inadequate cost-recovery results in an inability to operate and maintain supplies properly and will lead to increased leakage, interruptions and deterioration in quality & quantity | |
| |
· inadequate costs-recovery also prevents extension of services to unserved areas | |
| |
· poor cost-recovery may also lead to loss of water resources through pollution from inadequately treated wastewater | |
|
Recovering costs |
· costs recovered usually at least in part through levying of charge on consumers |
5,6 |
| |
· increasingly government support is being withdrawn from the sector which is expected to become self-financing | |
| |
· this may lead to reduction in programmes to extend coverage and disconnection for non-payment, both of which cause public health risks | |
| |
· it is essential that service provided is adequate to ensure costs may be recovered | |
| |
· this raises difficult questions such as whether service improvement or increased charges come first | |
| |
· arguments exist for both approaches, although it is clear that poor service will significantly limit cost recovery | |
| |
· community management can help reduce costs and assists in extending coverage | |
| |
· defaulters who can pay bills (e.g. government departments etc.) must be made to pay/the poor should not subsidise the rich | |
| |
· the need to pay should be promoted and the consumers made aware of the consequences of non-payment on service quality | |
|
Charging policies |
· these can be established in a number of ways |
7,8,9 |
| |
· key principle should be to ensure that water remains accessible and affordable to entire population |
|
| |
· charging should be fair and equitable and encourage conservation of water | |
| |
· rates or pay-per-use systems may be employed | |
| |
· pay-for-use systems require the installation of water meters |
|
|
|
· rates system usually work on property values as a mechanism of determining ability to pay | |
| |
· can use systems which employ elements of both approaches with minimum amount supplied at a flat rate and extra consumption charged per use |
|
|
|
· this protects poor whilst encouraging water conservation |
|
|
|
· problem is setting minimum to be supplied, although this should reflect health requirements | |
| |
· rate systems may use block rates or step rates | |
| |
· step rates employ increasing rates for increasing consumption and therefore promote conservation of water | |
| |
· block rates use decreasing rates for increasing consumption which penalises low-volume users | |
|
Keeping charges affordable |
· costs must kept affordable for all consumers in order to protect public health |
10 |
| |
· cross-subsidisation may be used | |
| |
· community operation and management will also reduce costs |
|
|
|
· industrial use of water can also be used to subsidise domestic use of water through use of differential tariffs | |
| |
· urban areas may subsidise rural areas as revenue generation easier in urban areas with larger, more concentrated populations | |
| |
· cost-recovery should also help to fund surveillance activities |
|
|
Non-payment issues |
· water suppliers may request on a policy of disconnection for non-payment as a means to ensure costs are recovered | |
| |
· however, there is no evidence of increased non-payment where disconnection is illegal and may reflect a desire for profit rather than cost recovery |
|
|
|
· disconnection causes serious public health risks and can never be recommended | |
| |
· for persistent non-payment, other options may include flow limitors | |
| |
· keeping costs affordable will reduce non-payment as an issue |
|
|
Conclusions |
· costs-recovery by some means is essential for sustainable water supply | |
| |
· government subsidy or application of differential tariffs may be employed to keep costs affordable | |
| |
· disconnection policies should not be implemented because of the public health risk | |
The Cost of Using Water (UK Example)
|
Flushing toilet |
1p |
|
Shower |
3.5p |
|
Dishwasher |
5.5p |
|
Bath |
8p |
|
Washing Machine |
11p |
|
Hose pipe (1 hour's use) |
54p |
(Assuming average cost of water, including disposal, of 0.1 pence per litre and typical consumption figures)
Investment Requirements
· Investment required in water supply and sanitation in lower income countries is approximately $50 billion per year.Actual spending is $10 billion per year.
(Christmas and LeRoy, 1990)
Consequence of Poor Cost-Recovery
· Inadequate cost-recovery will mean that water supply provision is not sustainable and will eventually lead to deterioration in infrastructure and human resources.
Water Supply Service Deterioration
Caused by Poor Cost-recovery and Cost Covering
Recovering Costs - Priorities
· Improved service quality or improved cost recovery?
Therefore:
» Does increased revenue fund service quality improvements?
or
» Do service quality improvements lead to increased revenue generation?
Sale price of water
World Bank (1990) reported that the average effective sale price of water is only about one-third of the marginal cost of production.
Charging Policies
Should aim to achieve:
· fairness and equity
· sensible incentives
· simplicity and comprehensibility
Keeping Water Charges Affordable
· Rich subsidise poor
· Community-based approaches
· Industry subsidises domestic
· Urban areas sinsidiserural
· How is surveillance funded? Water levy or other tax?
Nonpayment and Disconnection
· There is no evidence that disconnection policies have any impact on reducing non-payment of bills· Disconnection from a public water supply represents a serious public health risk
· Disconnection can never be justified on health grounds
Keeping charges affordable
· To protect public health costs must be affordable for all consumers· Cross-subsidation may be used
· Cost reduction may be achieved by community management and operation
· Industrial tariffs may subsidise domestic use
· Urban areas may subsidise rural ones
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Microbiology (Practical Exercise)
Session Objectives
· To discuss the relative advantages and disadvantages of the membrane filtration and multiple tube methods of analysis.· To provide participants with a practical experience of the membrane filtration technique.
· To provide participants with a practical example of the use of different volumes of filtration for different qualities of water.
· To review results and discuss precision of analysis.
Outline
NB: It is assumed that whoever takes this practical has a good working knowledge of microbiological techniques.
1. Collect two samples for testing (at least 1 litre of each) - one clean water and one contaminated water (from a river, stream, pond etc.).2. Demonstrate the membrane filtration technique and describe dilution methods (e.g. to make a 1 per cent solution add 1ml of sample to 99ml of distilled water).
3. Highlight the advantages and disadvantages of both the membrane filtration and the multiple tube methods of analysis.
4. Ask the participants to prepare and filter the following samples: 100ml; 50ml; 10ml; and 1ml.
5. Ask the participants to read the results the following day and record and compare the results.
6. A demonstration of other techniques - e.g. colilert - may also be given if resources permit.
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Disinfection (Practical Exercise)
Session Objectives
· To provide a practical example of how to calculate chlorine demand in a water supply.· To discuss and provide practical examples of different methods of chlorine residual analysis, with an emphasis on use of DPD tablets and comparators as a quick and reasonably accurate method.
· To discuss why free chlorine may be lost and the significance of high levels of combined chlorine.
Outline
NB:. It is assumed that whoever takes this practical has a good working knowledge of chlorine testing techniques and the relative advantages and disadvantages of different disinfectants.
1. Make up a range of chlorine solutions using HTH or chlorine tablets. It is suggested that 4-5 different concentrations of chlorine solution are prepared.2. Ask the participants to test the free and total chlorine residual in each solution and calculate the combined chlorine (combined chlorine = total residual - free residual).
3. Add contaminated water to solutions and ask the participants to re-test chlorine residuals.
4. Discuss the results and the need for maintaining residuals during distribution. Highlight the relative advantages and disadvantages of different disinfectants using the disinfectant session notes.
5. Discuss the ways in which free residual may be lost and highlight that highlight that high combined chlorine indicates sanitary integrity of the system is compromised.
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Sanitary Inspection (Practical Exercise)
Session Objectives
· To demonstrate the need for sanitary inspection in the management of water supplies.· To demonstrate the value of sanitary inspection as a means of promoting improvements in water supply.
· To describe the sanitary inspection techniques and the development of inspection forms based on risk scoring schemes.
Outline
1. Ask the participants, in small groups, to study the photographs and identify any sanitary risks present.2. Ask the groups to rank the systems. Make sure they do this independently and compare the findings of different groups.
3. Use these findings and the attached overheads to describe the key problems often faced with sanitary inspection.
4. Using the overheads, highlight that sanitary inspection data may be classified into broad groups indicating different levels of risk and that such data may also be used to rank systems on the basis of risk.
Participant Notes
1. Study the photographs carefully and note all the potential sanitary risks that you can identify.2. Rank the water supplies on the basis of greatest risk, with the supply at greatest risk first.
3. Briefly highlight some key common factors which should always be assessed when undertaking a sanitary inspection.
Typical Problems Preventing Effective Sanitary Inspection When Practiced
· No standardised methodology· Field interpretation of results varies between staff
· Data are difficult to quantify or compare due to subjectivity in interpretation and 'observational' style.
· No reporting structure to regional or national level
· No effort made to consolidate or analyse data at regional level in order to investigate general trends or common problems
Categories for Sanitary Inspection
|
Value |
Risk |
| |
|
|
0 |
No risk |
|
1-3 |
Little risk |
|
4-6 |
Intermediate risk |
|
7-10 |
High risk |
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Planning (Practical Exercise)
Session Objectives
· To provide a practical example of the process of planning water supply monitoring programmes which cover a wide range of conditions.· To reinforce the need to develop monitoring programmes which are linked to decision-making and management needs.
Outline
1. Divide the participants into at least two groups.2. Provide the participants with the attached description and ask one or more groups to design a health-based drinking-water quality surveillance programme for the town and the remaining groups to design a quality control monitoring programme for a water supplier.
3. Ask the groups to make a presentation on the programmes designed and discuss these in plenary.
NB: This practical is best run over several days. Therefore, the groups should be given the background information at the start of the workshop and asked to present their findings on the last day.
Monitoring Programme Design
The town of Terebaka serves a total population of 105,000. The town is a regional centre of importance and has a busy market selling foodstuffs and a variety of hardware and clothes and an industrial area. The town is the centre for the surrounding district and the population is significantly increased on market days. The town is also an important rail and bus terminus and the short-term transient population is high.
The town has a centralised piped water supply which serves 85 per cent of the population with a mixture of in-house and yard level water supply service (roughly a 40-60 split). In addition, a number of public tapstands are located in the market and at the bus and rail stations. The piped water supply utilises two main sources: a reservoir situated 20 kilometres to the north of the town and connected to the water treatment plant; and a well field (series of boreholes) 10 kilometres to the west of the town which joins the distribution system at the major storage tank on the western extremity of the town.
The treatment plant utilises coagulation-flocculation-settling through two conventional settlers set in parallel. This is followed by rapid sand filtration and the plant has two filters per settler. The water is disinfected with hypochlorite does through a pulse doser into the final clear well. The water is then pumped to the main town storage tank which feeds the distribution systems which passes through 6 subsidiary tanks spread around the city.
The well field water is pumped to a central collector tank where it is chlorinated using a gas chlorinator and the water is then pumped to the major tank on the west of the city, form where the water is distributed through the main system.
The treatment plant has suffered a number of failures during the recent past and the coagulation-flocculation-settling in particular is known to be inefficient. Problems have arisen through the lack of coagulant and insufficient settling time. Some problems have also been encountered with the chlorination of water form both sources.
The distribution system is old and has a leakage rate of around 3- per cent. Several "hotspots" of pipe leakage are known and there are also several areas of known low pressure within the system.
The parts of the town not served by the main pipe system are on the periphery of the town and utilise hand-dug wells in most areas, although several private boreholes have been sunk.
Design a monitoring scheme for Terebaka, indicating the range of analysis, frequency of sampling, type of sampling points, location of sampling points and frequency of sanitary inspection. Indicate the objectives of your monitoring programme and highlight the actions you would take on the basis of the results received.

Figure

Figure

Figure

Figure

Figure
Figure
Figure
Figure

Figure

Figure