| Fact sheet No 095: Onchocerciasis (River Blindness) - Revised February 2000 (WHO, 2000, 4 p.) | |||
| (introduction...) | |||
| Onchocerciasis (River Blindness) | |||
|
| ||||||||||||
Onchocerciasis - the world’s second leading infectious cause of blindness - is present in 36 countries of Africa, the Arabian peninsula and the Americas. As a public health problem the disease is most closely associated with Africa, where it constitutes a serious obstacle to socio-economic development. Onchocerciasis is often called “river blindness” because of its most extreme manifestation and because the blackfly vector abounds in fertile riverside areas, which frequently remain uninhabited for fear of infection.
Prevalence
Out of some 120 million people world-wide who are at risk of onchocerciasis, 96% are in Africa.Of the 36 countries where the disease is endemic, 30 are in sub-Sahara Africa (plus Yemen) and six are in the Americas.
A total of 18 million people are infected with the disease and have dermal microfilariae, of whom 99% are in Africa.
Of those infected with the disease, over 6.5 million suffer from severe itching or dermatitis and 270 000 are blind.
Characteristics
Onchocerciasis is caused by Onchocerca volvulus, a parasitic worm that lives for up to 14 years in the human body. Each adult female worm, thin but more than 1/2 metre in length, produces millions of microfilariae (microscopic larvae) that migrate throughout the body and give rise to a variety of symptoms: serious visual impairment, including blindness; rashes, lesions, intense itching and depigmentation of the skin; lymphadenitis, which results in hanging groins and elephantiasis of the genitals; and general debilitation. Onchocerciasis manifestations begin to occur in persons one to three years after the injection of infective larvae.
Microfilariae produced in one person are carried to another by the blackfly, which in West Africa belongs to the Simulium damnosum species complex. The blackfly lays its eggs in the water of fast-flowing rivers. Adults emerge after 8-12 days and live for up to four weeks, during which they can cover hundreds of kilometres in flight.
After mating, the female blackfly seeks a bloodmeal and may ingest microfilariae if the meal is taken from a person infected with onchocerciasis. A few of these microfilariae may transform into infective larvae within the blackfly, which are then injected into the person from whom the next meal is taken and subsequently develop into adult parasites, thus completing the life cycle of the parasite.
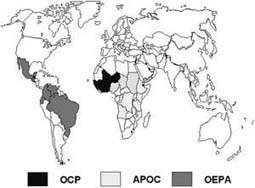
The Onchocerciasis Control Programme (OCP)
OCP was the first major programme developed to control onchocerciasis. It was launched in 1974 in an area that originally encompassed seven countries in West Africa. In 1986 the programme was extended to include four additional countries, bringing the current total of participating countries to 11. The total operational area covers 1.23 million sq. km and a combined population of about 30 million people.
The programme has been jointly sponsored by WHO, the World Bank, the United Nations Development Programme and the Food and Agriculture Organization and is supported by a coalition of more than 20 donor countries and agencies. WHO acts as the Executive Agency for the programme, while the World Bank is responsible for mobilizing resources and administering the OCP Trust Fund. The Programme is scheduled to come to an end by the year 2002. The estimated total cost for the programme will be US$550 million, or less than US$1 per year for each protected person.
OCP’s principal method for controlling onchocerciasis has been to break the cycle of transmission by eliminating the black fly. Simulium larvae are destroyed by application of selected insecticides through aerial spraying of breeding sites in fast-flowing rivers. Once the cycle of river blindness has been interrupted for 14 years the reservoir of adult worms dies out in the human population, thus eliminating the source of the disease. The parasite reservoir has now virtually died out in the original 7-country operations area (map) and will be largely eliminated in the remaining four countries by the year 2002. To complement vector control activities, OCP now distributes the drug ivermectin where needed in the operations area through a community directed approach. Ivermectin kills the larval worms that cause blindness and other onchocercal manifestations and acts to decrease transmission as well.
Programme Achievements
At OCP’s launch, more than 1 million people in West Africa suffered from onchocerciasis, of whom 100 000 had serious eye problems including 35 000 people who were blind. Today, the number of infected people within the original area of operations is practically nil and vector control efforts have almost ceased.Some 1.5 million people who were once infected with onchocerciasis no longer have any trace of the disease. Eleven million children born in the operational area since the programme’s inception are now free of risk of contracting the disease.
At the turn of the century it was estimated that OCP had prevented almost 300 000 cases of blindness in the 11 countries involved in the programme.
The successful vector control activities are opening up an estimated 25 million hectares of fertile riverine land for resettlement and cultivation, land that was previously deserted for fear of onchocerciasis. This land has the potential to feed an additional 17 million people annually through the use of indigenous technologies and farming practices.
Global Control Strategy
The development of ivermectin in the 1980’s provided for the first time a safe, effective drug capable of reducing the numbers of skin microfilariae in infected people and resulting in clinical improvement and decreased transmission of infection. As a result, a new global strategy for controlling onchocerciasis has now been defined that is based on:
yearly administration of single doses of ivermectin to affected populations.
In 1987 ivermectin’s manufacturer, Merck & Co., Inc., pledged to provide at no cost all the drug necessary for as long as necessary to overcome onchocerciasis as a public health problem. It established the Mectizan® Donation Program which has collaborated with WHO, health ministries and non-governmental development organizations (NGDOs) so that between 1987 and the end of 1996, more than 65 million doses of Mectizan® had been donated for distribution.
Onchocerciasis Elimination Program in the Americas (OEPA)
To coordinate onchocerciasis control efforts in the 6 endemic countries of the Americas and to reach the goal of eliminating first the pathology and then the disease, the Onchocerciasis Elimination Programme for the Americas (OEPA) was created in 1992 with the support of PAHO, the Inter-American Development Bank, a consortium of NGDOs, and all of the affected countries.
The African Programme for Onchocerciasis Control (APOC)
The outstanding success of the Onchocerciasis Control Programme (OCP), when expressed in health, economic and development terms, was the motivating rationale for the launching of a new programme, African Programme for Onchocerciasis Control (APOC) in December 1995. APOC shares the same co-sponsoring agencies and donors with the OCP.
Unlike the OCP, the new Programme, APOC is non-vertical and based on a full partnership between affected communities, the participating governments, a consortium of international non-governmental development organizations (NGDOs) and bilateral agencies.
The Programme’s objective is to establish, within a period of 12 years, sustainable community-directed ivermectin (Mectizan®) distribution systems covering about 50 million people in 19 countries outside the OCP where onchocerciasis still is a serious public health problem. These countries are: Angola, Burundi, Cameroon, Chad, the Central African Republic (CAR), the Congo, the Democratic Republic of the Congo, Ethiopia, Equatorial-Guinea, Gabon, Kenya, Liberia, Malawi, Mozambique, Nigeria, Rwanda, Uganda, Sudan and Tanzania.
In these countries, it is estimated that of the 15 million heavily infected people, 6.4 million live in areas where the parasite strains are a major cause of blindness while 8.6 million live in areas where the parasite strains are responsible for severe skin disease associated with grave and unrelenting itching.
APOC partners share responsibilities in implementing the Programme’s principal control strategy which is based on community directed treatment with ivermectin (CDTI). Where feasible, ivermectin treatment will be complemented with vector elimination using environmentally safe methods.
Since its inception, the Programme management has been set up at the OCP headquarters and National Onchocerciasis Task Forces (NOTF) have been created in 14 countries. The Memorandum (a multilateral agreement) has been signed by 19 countries and 13 donors bringing the programme legally into force as of April 1996. At the end of 1999, 12 national plans for the control of onchocerciasis had been developed and 57 projects were approved for funding, including: ivermectin distribution projects (48), vector elimination projects (4) and projects for strengthening NOTFs’ secretariats (5). Thirty-eight of these projects have already been started.
In 1996, the NGDO Coordination Group facilitated distribution to 7.5 million people. This number increased to 11.7 million in the first year of APOC’s field activities (1997-1998) and was expected to rise to over 15 million by the end of 1999. This constant increase, as well as close working relationships amongst all APOC partners will enable APOC to achieve its goal of treating about 45 million people by the year 2007.
Challenges ahead for OCP and APOC
When OCP comes to an end in the year 2002, its present strategy of aerial larviciding will no longer be applicable. However, some OCP countries are already benefiting from ivermectin distribution as the only control method. These will continue with ivermectin treatment, sharing the same control strategy and challenges with APOC. The challenges include:
Onchocerciasis control programme(i) Developing with the affected communities, competent delivery systems to serve as example for the delivery of other drugs to control other tropical diseases.
(ii) While the OCP towards its end is aiming at having the devolved activities integrated into the varied health systems, APOC is aiming at devolving all aspects of control operations into the health systems from the onset, in participating countries. The two programmes will share experiences on this issue.
(iii) Finally, APOC has an additional challenge, to demonstrate the effectiveness of its unique partnership in implementing a sustainable solution to a public health and development problem.
For further information in Geneva, please contact: in Geneva - WHO Office of Press and Public Relations, Tel. (+41 22) 791 2599, Fax (4122) 791 4858, e-mail inf@who.int. In Burkina Faso: Dr K.Y. Dadzie, Director, Onchocerciasis Control Programme; and Acting Director, African Programme for Onchocerciasis Control, Tel. (226) 30 23 01, Fax (226) 30 21 47.
All WHO Press Releases, Fact Sheets and Features as well as other information on this subject can be obtained on Internet on the WHO home page https://www.who.int